

Pectus excavatum symptoms may be absent in mild cases. When present, they are often related to exercise, breathing difficulties, or chest discomfort. Symptoms to watch for include:
Seek medical attention promptly if pectus excavatum chest pain is severe, if you faint, or if you develop significant breathlessness that is new or worsening.
The risk factors for pectus excavatum are associated with:
You should see a thoracic surgeon or lung specialist when pectus excavatum causes symptoms, worsens, or affects your daily life or confidence. It is also reasonable to seek a review if the chest depression appears to deepen during growth, or if you want an objective assessment before deciding whether to monitor or treat.
In Singapore, many patients start with a family doctor, a school health referral, or a routine scan that detects an abnormal chest shape. Others self-refer to a private specialist to secure a clear plan without delay.
If you are seeing multiple providers, a thoracic surgery specialist can coordinate your care and interpret your results in context.
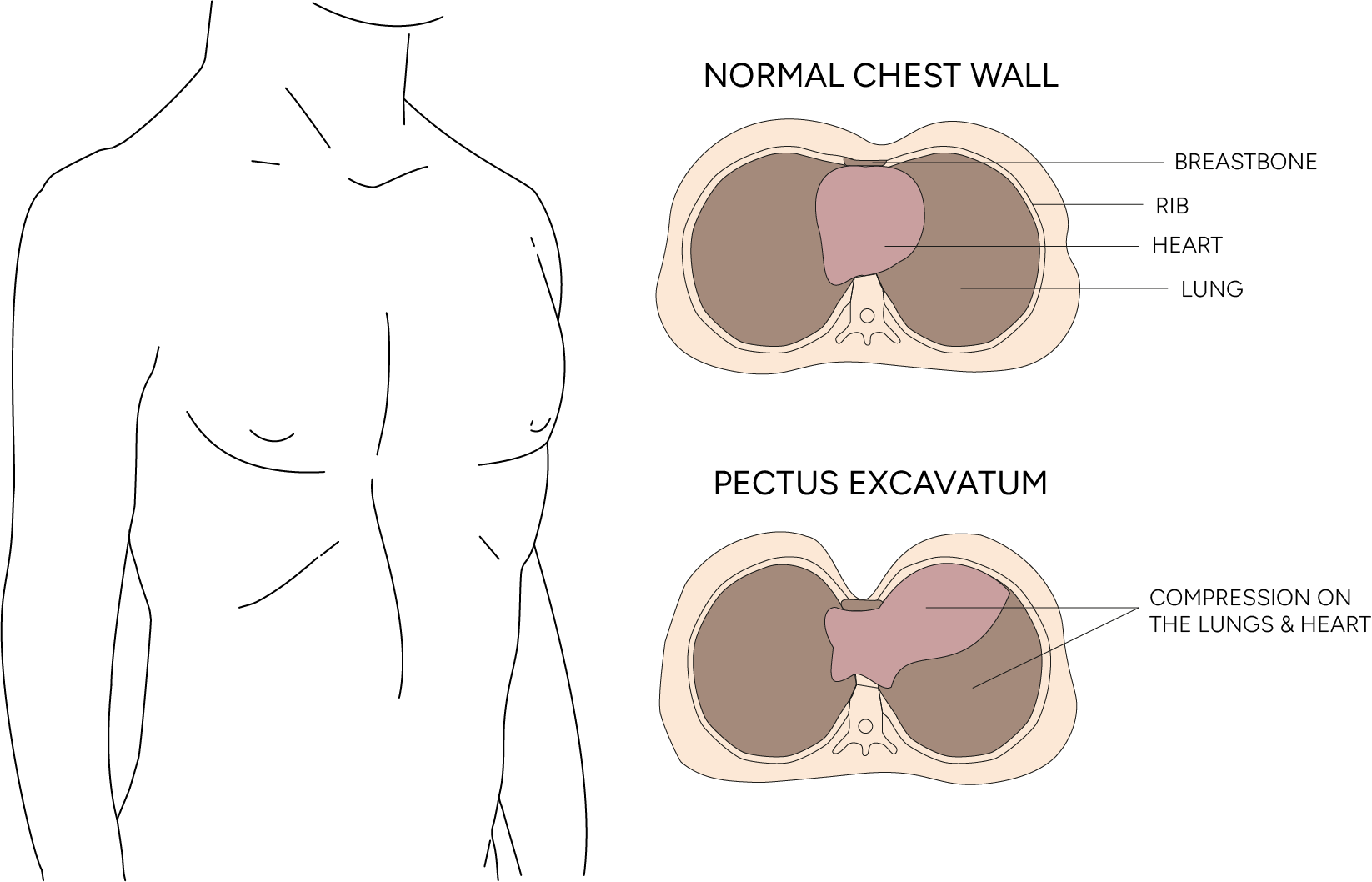
Diagnosis for pectus excavatum begins with a physical examination and is confirmed by imaging and functional tests when indicated. The first step is usually a detailed history, including exercise tolerance, chest pain, breathlessness, and any family history of chest wall conditions and connective tissue disorders. Your clinician will assess chest shape, posture, and any associated rib flare or asymmetry, including asymmetric pectus excavatum, in which one side of the chest is more affected.
Tests may include the following:
Not every patient needs every test. The aim is to answer practical questions: how severe is it, does it affect heart and lung function, is it stable, and what are the treatment options? Pectus carinatum, the opposite condition where the breastbone protrudes, may also be assessed during the same evaluation.

In children and teenagers, pectus excavatum often becomes more noticeable during puberty and may progress as the child’s chest grows. Many young people have mild pectus excavatum that does not cause physical limitations. Others develop symptoms with sport, or feel distressed about appearance at a time when body image matters deeply. Older children approaching adolescence should be monitored if the child’s chest shape is changing.
A paediatric- or adolescent-focused assessment evaluates the growth stage, trends in severity, and functional impact. Timing can matter for pediatric surgery. Some surgical approaches are commonly considered during adolescence because the chest wall is more flexible and outcomes are more predictable; however, the optimal timing is individualised, depending on symptom burden and family preferences. Pediatric surgery for funnel chest is one of the most well-studied corrective procedures in thoracic surgery.
A common local point in Singapore is fitness testing. Some families first notice a limitation when a teenager struggles to keep up in school, sports, doing their NAPFA or IPPT, or during National Service pre-enlistment fitness preparation. That is not diagnostic on its own, but it can prompt a useful, objective workup.

Non-surgical treatment can help mild pectus excavatum and support recovery even when surgery is planned. Conservative treatment is often the first step for mild cases without cardiopulmonary effects, focusing on posture, breathing mechanics, and strength.
Non-surgical options may include:
The vacuum bell is a common, non-surgical tool used to treat a sunken chest. It uses suction to pull the breastbone forward. It is most effective for younger patients whose chest remains flexible. Regular use can gradually improve the condition, but it may not be sufficient for severe cases. A physician should monitor patients using the device, which is sometimes used alongside physical therapy.
Non-surgical treatment and conservative treatment approaches do not alter the underlying cartilage growth pattern in the same way surgery can, but they can improve function, confidence and chest appearance in mild cases.

Surgery is generally recommended as a pectus excavatum cure if it is moderate to severe, causes problems like breathing or heart issues, or greatly affects how a person feels about themselves. For severe cases, surgery is usually the best way to correct a sunken chest. The decision to operate depends on multiple factors, not just a single test result.
The Nuss procedure for pectus excavatum is a keyhole, minimally invasive repair. It was developed by Dr Donald Nuss in the 1980s and is now the main surgical treatment for pectus excavatum globally.
During surgery, the doctor makes small incisions on each side to insert a curved metal bar (a ‘pectus bar’) beneath the breastbone. Using a tiny camera for guidance, the surgeon places the bar to gently push the sunken breastbone and cartilage outward to a normal position. Sometimes more than one bar is needed. The bar stays in to reshape the chest wall over time. The surgery takes 1-2 hours under general anaesthesia.
The biggest benefit of Nuss bar fixation using ZipFix is its minimal invasiveness. Unlike open surgeries, it uses small incisions, resulting in less pain, shorter hospital stays, and faster recovery.
The Ravitch procedure is an open chest surgery to fix pectus excavatum. The surgeon makes an incision, removes the abnormal cartilage, and uses medical devices to move the breastbone into a better position. This method is often chosen for specific chest shapes, chest asymmetry, or prior surgery.
Your surgeon will discuss the best repair technique for your body and goals.

Thoracic surgery experience is important because pectus excavatum repair requires operative access to the heart, lungs, and major blood vessels. At Neumark, we utilise minimally invasive thoracic surgery techniques and careful planning to support safe access, precise dissection, and a structured recovery pathway. The approach is always chosen for safety and suitability, not for novelty.
Most patients recover well, but pectus excavatum surgery still requires a realistic recovery plan.
Risk factors include age, body type, and prior chest surgery. Your surgeon will discuss your specific risk profile. Common considerations include bleeding, infection, pneumonia, air leak, and fluid collections. In bar-based repair, bar displacement is a known risk, although careful fixation reduces it. Some patients develop longer-lasting pain or numbness around the small incision sites. Rarely, serious complications can occur due to the proximity to the heart and lungs, which is why experienced thoracic surgery planning and intraoperative safeguards matter.
Pain management is central to recovery. Many patients undergo a structured pain management plan that may include multimodal pain medication and, in selected cases, regional anaesthesia techniques. Early mobilisation and breathing exercises help reduce the risk of complications.
Here is what to expect for recovery:
Your team will provide guidance on posture, sleeping positions, activity restrictions, and when it is safe to return to school, work and exercise.

Recurrence is uncommon but can occur, especially if the surgical repair is performed very early, the chest wall continues to grow significantly during a growth spurt, or the repair is complicated by bar displacement.
Following recovery advice and attending follow-up visits reduces risk. For bar-based repairs, bar removal is planned at the appropriate time, and timing is critical to maintaining correction. For surgically treated pectus excavatum, ongoing monitoring of the heart and lungs is essential to ensure durable outcomes.
Long-term outcomes depend on the initial severity, the technique used, and the individual’s health. Many patients experience improved exercise tolerance and comfort after successful repair of pectus excavatum. Even when the function is normal, correcting severe deformity can meaningfully improve confidence and daily well-being.
The cost of pectus excavatum surgery in Singapore depends on the procedure recommended, the length of the hospital stay, the surgeon’s fees, the implants used, and insurance coverage. Many insurance plans may cover medically necessary chest wall surgery, but coverage varies by policy and often requires pre-authorisation and supporting clinical documentation. Your thoracic surgery team can provide a detailed estimate and advise you on the paperwork your insurer may require at the consultation.
Neumark Lung & Chest Surgery Centre offers expert assessment, testing and treatment plans for pectus excavatum in Singapore. We provide both non-surgical and surgical options.
Dr Harish Mithiran, a senior thoracic surgeon at Gleneagles and Mount Alvernia hospitals, leads care at our specialised clinic, specialising in both child and adult pectus excavatum surgery. His focus is on accurate diagnosis, honest discussion of options, and evidence-based recommendations. When surgery is necessary, Neumark supports decision-making, explains the techniques involved, and facilitates recovery through a team approach.
If you or your child has a sunken chest and you want a clear check of its severity, symptoms, and treatment options, contact Neumark Lung and Chest Surgery Centre to book an appointment at Gleneagles or Mount Alvernia Hospital.