

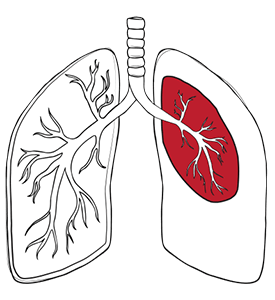
There are multiple types of pneumothorax:
A spontaneous pneumothorax happens without an external injury. Primary spontaneous pneumothorax usually occurs in people without known lung disease, often because small blebs or bullae near the top of the lung rupture.
A secondary spontaneous pneumothorax happens in someone with an underlying lung disease such as a chronic obstructive pulmonary disease (COPD), emphysema, cystic fibrosis, pneumonia, lung cancer, or certain cystic lung disorders.
A traumatic pneumothorax may be due to a chest injury such as a rib fracture, knife wound, or blunt trauma to the chest, while an iatrogenic pneumothorax happens after a medical procedure such as a lung biopsy or central line insertion.
An open pneumothorax occurs when a chest wall opening allows outside air to enter the pleural space.
A closed pneumothorax means the chest wall remains intact and the air leak comes from the lung itself.
A tension pneumothorax is a dangerous condition in which air enters through a one-way valve mechanism in the chest wall or lung, so the air cannot escape from the pleural space, causing pressure to rise inside the chest, shifting the mediastinum, and quickly leading to respiratory failure and cardiovascular collapse. This is a life-threatening emergency.
A rare catamenial pneumothorax can occur in women around menstruation and is linked with thoracic endometriosis.
Pneumothorax symptoms usually start suddenly and most often include chest pain and shortness of breath.
The pain is often sharp and may worsen with breathing. Difficulty breathing is one of the hallmark symptoms of a collapsed lung and should prompt immediate medical attention. Some people also develop a cough, rapid breathing, a rapid heart rate, fatigue, or a bluish tinge to the lips or skin when their lungs are not exchanging oxygen properly. Symptoms are often more severe when a larger portion of the lung has collapsed or when the person already has underlying lung disease.
In a small spontaneous case, the person may feel only mild discomfort. Symptoms of a small closed pneumothorax may include only minor chest pain and slight difficulty breathing. In a tension pneumothorax, difficulty breathing can worsen quickly and may be accompanied by severe distress, low blood pressure, and signs of shock.
In an open pneumothorax, there may be a visible chest wound with significant difficulty breathing. If you notice your breathing becoming more laboured or your lungs not filling properly, these may be symptoms of a pneumothorax that requires urgent care.

A pneumothorax can occur when air leaks from the lung, enters through the chest wall, or builds up after injury, disease, or a medical procedure. Common causes and risk factors include:
You should seek urgent medical attention for a suspected pneumothorax, and a thoracic specialist review is especially important when symptoms are severe, the lung does not re-expand, or the condition recurs.
A suspected pneumothorax is not something to monitor at home without assessment. Even if the lung collapse turns out to be small, the same symptoms of a collapsed lung can also occur in other serious chest emergencies.
A pneumothorax is an emergency when chest pain is severe, breathing becomes difficult, or symptoms worsen quickly.
Seek urgent care if you have:
A thoracic surgeon’s review is particularly important in recurrent pneumothorax, a persistent air leak, pneumothorax in both lungs, traumatic cases, or when a chest tube does not allow the lung to expand properly. If you have had a collapsed lung before, if you have underlying lung diseases, or if you work in a high-risk occupation, speaking with a doctor early is essential. Specialist input is also helpful for those whose work or lifestyle puts them at an increased risk of recurrence, such as pilots, cabin crew or divers. At Neumark Lung & Chest Surgery Centre, decisions about observation, chest drainage, pleurodesis, or minimally invasive surgery become more precise and individualised.
Pneumothorax treatment without surgery is often possible when the collapse is small, symptoms are mild, and the lung is likely to re-expand safely. Not every pneumothorax needs an operation. Some small cases are managed with observation, repeat imaging, and sometimes oxygen therapy while the body gradually reabsorbs the air into the pleural space. A pneumothorax can resolve without surgery in selected cases, but a doctor still needs to confirm that it is safe to take that approach. Pneumothorax treatment depends on the size of the collapse, symptoms, cause, and whether it has happened before.
For small, stable pneumothorax without severe symptoms.
May help the body reabsorb air more quickly in selected cases.
For selected larger primary spontaneous pneumothorax or symptomatic cases.
For larger pneumothorax, secondary pneumothorax, persistent air leak, traumatic pneumothorax, or unstable patients.
For recurrence prevention in selected cases.
For recurrent pneumothorax, persistent air leak, bilateral pneumothorax, failure of lung re-expansion, traumatic lung injury, or high-risk occupations.

Pneumothorax surgery is usually recommended when the air leak does not stop, the lung fails to re-expand, the pneumothorax recurs, or the risk of recurrence is particularly high.
Common reasons include a persistent air leak from a chest tube, failure of the lung to expand, recurrent collapsed lung, pneumothorax in both lungs, traumatic injury, or occupational reasons such as professional flying or diving. The aim is to reduce the likelihood of a collapsed lung occurring again.
At Neumark Lung & Chest Surgery Centre, surgery for spontaneous and recurrent pneumothorax is centred on minimally invasive thoracic surgery techniques.
Video-Assisted Thoracoscopic Surgery (VATS) allows the surgeon to enter the chest cavity through small incisions using a camera and long instruments. Uniportal VATS uses a single small incision and is part of Neumark’s minimally invasive practice. During VATS or U-VATS surgery, the surgeon looks for the leaking area, often a bleb or bulla near the top of the lung. The leaking portion may be removed with a stapling device. A pleural procedure, such as pleurodesis or pleurectomy, may then be performed to help the lung stick to the chest wall and reduce the chance of recurrence. This combination is especially relevant in spontaneous or recurrent pneumothorax. Surgery lowers the risk of recurrence in eligible patients, but it cannot eliminate every possible cause of a future air leak.
Robotic-Assisted Thoracic Surgery (RATS) is a powerful tool in many chest operations, but it is not the standard first-choice operation for most pneumothorax cases.
In routine pneumothorax surgery, VATS or U-VATS is usually more relevant. The procedure chosen depends on the disease pattern, prior episodes, lung condition, and the surgeon’s judgement about which approach will most effectively seal the leak while keeping the operation as minimally invasive as possible.

Most people recover well after treatment for a pneumothorax, but recovery depends on the cause, treatment used, and risk of recurrence.

Neumark Lung & Chest Surgery Centre can help by assessing the cause of the pneumothorax, choosing the safest treatment, and, where possible, reducing the risk of future episodes.
Neumark specialises in minimally invasive thoracic surgery with a multidisciplinary approach led by Dr Harish Mithiran, senior consultant thoracic surgeon at Gleneagles and Mount Alvernia hospitals. We will review your imaging and history carefully before recommending a treatment plan.
If surgery is needed, Neumark’s approach emphasises minimally invasive techniques, such as VATS and U-VATS, to repair the air leak and reduce the risk of recurrence in patients with pneumothorax, while minimising surgical trauma. If surgery is not needed, the focus remains on safe drainage, recovery, follow-up imaging, and prevention of future episodes.
If you or a loved one has been diagnosed with a pneumothorax, or if you have sudden chest pain and difficulty breathing that could be a collapsed lung, contact Neumark for a consultation.

