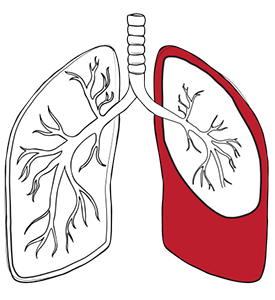


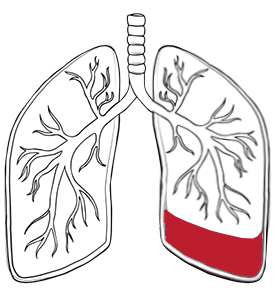
Pleural effusions are classified into distinct categories based on the fluid’s composition and underlying causes to help determine the most appropriate treatment approach:

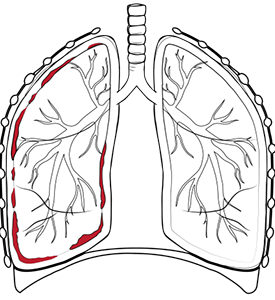
Symptoms of pleural effusion vary considerably depending on the volume of fluid accumulation and the underlying cause. The greater the build-up of fluid, the more likely symptoms will be noticeable. Many patients initially dismiss early symptoms as common respiratory complaints, delaying crucial diagnosis and treatment.
Common symptoms include progressive shortness of breath, particularly during physical activity or when lying flat. Chest pain often presents as a sharp pain that worsens with deep breathing or coughing. A persistent dry cough may develop as the body attempts to clear a perceived obstruction.
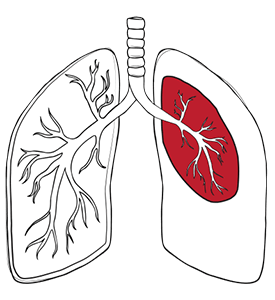
In extreme cases, a person can have up to four litres of excess fluid in the chest, making breathing extremely uncomfortable. Patients frequently describe feeling as though something is pressing against their chest, preventing them from fully expanding their lungs.
Additional symptoms may include fever, particularly when the infection causes the effusion, and general fatigue resulting from compromised oxygen exchange. Some individuals experience reduced exercise tolerance and difficulty sleeping due to breathing difficulties when lying down. A prompt medical evaluation is essential for an accurate diagnosis and effective treatment.

Pleural effusion is not a condition in itself but a symptom of an underlying disease. Among the most common causes of pleural effusion are:
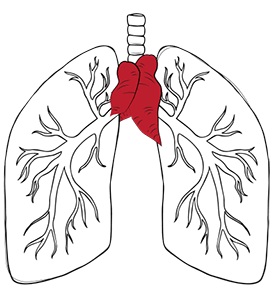
Some people have more than one of the causes above. The most common causes include heart failure, which accounts for a significant proportion of transudative effusions. When the heart cannot pump effectively, fluid backs up into the lungs and surrounding tissues, sometimes resulting in pulmonary oedema.
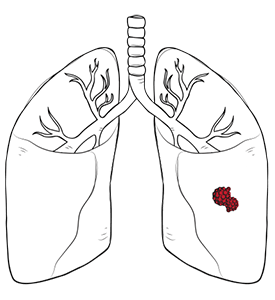
Cancer represents another major cause, either through direct tumour involvement or as a side effect of treatment. Malignant pleural effusion often indicates advanced disease and requires specialised oncological management alongside treatment for pleural effusion.
Infections, particularly pneumonia and tuberculosis, can trigger inflammatory responses leading to fluid accumulation. Liver disease, kidney failure, and autoimmune conditions such as inflammatory bowel disease also contribute to pleural effusion. Lung injury, ovarian hyperstimulation syndrome and oesophageal rupture are additional potential causes that should be considered in the differential diagnosis.
Less common examples of what can cause a pleural effusion include pulmonary embolism, medication reactions and trauma. Identifying the cause of pleural effusion is essential for management. Identifying the underlying cause is crucial for developing an effective treatment strategy and preventing recurrence.

There are several treatment options for pleural effusion, depending on the underlying cause and severity. In many cases, especially with smaller effusions, conservative treatment and medication may be sufficient. Diuretics can be used for effusions caused by heart failure, while antibiotics may be prescribed for those resulting from infections.
When fluid continues to build or causes significant discomfort, draining fluid from the chest cavity becomes a key step in management. This can be done through repeated thoracentesis or by inserting chest tubes to remove fluid over time. Chest tubes are commonly used in the management of pleural diseases, especially when larger volumes need to be drained or when ongoing drainage is required. For recurrent or complex cases, surgical intervention may be necessary.

At Neumark, video-assisted thoracic surgery (VATS) is a minimally invasive option for pleural effusions that need more than simple drainage. This approach is used to diagnose the cause of the fluid, perform pleurodesis to prevent recurrence, clear complex or loculated fluid, and release trapped lung caused by scarring. Through small incisions, surgeons can visualise the chest cavity and address multiple issues in a single procedure. Patients often experience less pain, shorter hospital stays, and a quicker recovery compared to traditional open surgery.

In certain complex cases, a traditional thoracotomy may still be necessary. This open surgical approach enables more extensive procedures, such as decortication (the removal of fibrous tissue that restricts lung expansion) or a full exploration of the pleural cavity in cases of difficult infections or malignancies. The decision between VATS and thoracotomy is made carefully based on the patient’s specific condition and overall health.

Pleural effusions can sometimes lead to serious complications if not managed promptly and effectively. One of the most significant risks is respiratory failure, which can occur if excess fluid in the pleural space severely restricts lung expansion. In rare cases, large or rapidly accumulating pleural effusions may also put pressure on the heart, leading to a life-threatening condition known as cardiac tamponade. Another potential complication is empyema, where infection causes pus to collect in the pleural cavity, often requiring urgent intervention.
The prognosis for pleural effusions varies widely and is closely linked to the underlying cause and the speed with which treatment is initiated. For example, malignant pleural effusions, often associated with advanced lung cancer or metastatic disease, tend to have a poorer outlook, with median survival rates typically ranging from four to six months. In contrast, transudative pleural effusions resulting from conditions like congestive heart failure or a pulmonary embolism can have a much better prognosis, especially when the underlying heart failure or clot is treated effectively.
Accurate diagnosis of pleural effusion is crucial for determining the most effective course of action and predicting outcomes. Pleural fluid analysis, including measurements of pleural fluid protein and lactate dehydrogenase (LDH), helps differentiate between complicated vs uncomplicated pleural effusions, guiding further management. In some cases, additional procedures such as pleural biopsy or the placement of an indwelling pleural catheter may be necessary to both diagnose and treat persistent or complicated pleural effusions. When infection or malignancy is involved, more aggressive treatments like chest tube drainage and targeted antibiotics or cancer therapies may be required.
Ultimately, early recognition and comprehensive evaluation are key to improving prognosis and reducing the risk of complications in patients with pleural effusions.

Recovery time varies significantly based on the chosen treatment approach. After thoracentesis, patients may need to take it easy for two days, whilst VATS requires a few days of hospitalisation. Traditional thoracotomy typically requires approximately one week of hospital stay.
Postoperative care includes pain management, respiratory therapy and a gradual progression of activity. Patients receive detailed instructions on wound care, activity restrictions and signs of complications that require immediate medical attention.
Long-term management requires regular follow-up appointments to monitor for the redevelopment of effusion and assess the effectiveness of treatment.

Preventing the recurrence of pleural effusion largely depends on addressing the underlying cause. For example, in malignant effusions, repeated fluid accumulation can be managed through the use of indwelling pleural catheters or chemical pleurodesis. For infectious causes, complete treatment of the infection is crucial.
Lifestyle adjustments may also play a role, particularly in managing heart or kidney conditions that can lead to recurrent fluid retention. Our team at Neumark offers long-term follow-up and monitoring, ensuring patients receive comprehensive care even after the initial treatment.