

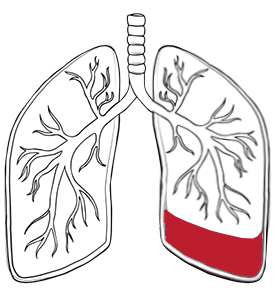
The main types of pleural effusion are transudative and exudative, and the difference helps guide treatment.
A transudative pleural effusion happens when pressure changes in blood vessels cause watery fluid to leak into the pleural space. The fluid accumulates within intact blood vessels, and the visceral and parietal pleura remain uninflamed. Common pleural effusion causes of this type include congestive heart failure, liver cirrhosis, kidney disease, peritoneal dialysis and low blood protein levels.
On the other hand, an exudative pleural effusion occurs when inflammation, infection, cancer or pleural disease increases the permeability of the visceral and parietal pleura, allowing protein-rich pleural fluid to accumulate.
This distinction matters because the underlying cause changes the treatment plan. Transudative effusions often improve when the underlying systemic problem is controlled. An exudative effusion usually requires further investigation and may require drainage, biopsy, or surgery.

Pleural effusion symptoms depend on the amount of pleural fluid, how quickly it develops, and the cause.
The most common symptoms of pleural effusion are shortness of breath, chest pain and a cough. Some patients describe a heavy feeling in the chest. Shortness of breath and chest pain together are characteristic presenting features of pleural effusion, causing respiratory symptoms. If the pleural fluid accumulates slowly, symptoms of pleural effusion may remain mild until the fluid accumulation becomes substantial. If it builds up quickly, even a smaller pleural fluid buildup can feel dramatic.
The signs of pleural effusion on examination may include reduced breath sounds, dullness to percussion, and reduced chest movement on the affected side. Imaging is still needed to confirm the presence of pleural fluid and estimate its volume.
The symptoms can also reflect the underlying cause. Fever, chills, and feeling unwell may point towards an infection. Weight loss or recurrent pleural fluid accumulation may suggest malignancy. Swollen legs and shortness of breath when lying flat may be more consistent with heart failure. This is why pleural effusion should never be treated as just a fluid problem. The pleural fluid is only part of the story; the underlying cause needs to be addressed.
Diagnosis of pleural effusion begins with imaging and often requires pleural fluid analysis to identify the cause.
A medical history review and careful blood tests are essential early steps. Blood tests can reveal heart failure, kidney disease, or autoimmune conditions. Medical history often guides further pleural fluid analysis.
A chest X-ray is often the first clue. It may show blunting of the costophrenic angle, which is the anatomical junction where the chest wall meets the diaphragm, a meniscus of fluid, or a more extensive white-out if the effusion is large. An ultrasound scan is more sensitive than an X-ray for detecting smaller collections and is useful for safely guiding the drainage. Computed tomography (CT) scanning is especially helpful when the pleural fluid is complex, malignancy is suspected, or pleural thickening, loculations, trapped lung, or other thoracic conditions need to be assessed. CT scans also help identify blood clots and blood vessels affected by the disease process.
A key part of pleural effusion diagnosis is thoracentesis, also called a pleural tap. This involves using a needle to remove the pleural fluid for analysis. The pleural fluid is tested for protein, lactate dehydrogenase, pH, glucose, cell count, microbiology, and, where appropriate, pleural fluid cytology. Pleural fluid analysis and pleural fluid cytology together help determine whether the pleural fluid is transudative or exudative and narrow the list of causes of pleural effusion. Pleural fluid drainage during thoracentesis can also provide immediate symptom relief.
Some patients need more than a pleural fluid analysis. If the pleural fluid recurs, if the pleural fluid cytology is negative but malignancy remains a concern, or if the infection appears organised, doctors may recommend a pleural biopsy or thoracoscopy. The results of these biopsies are essential to guide further management.
The cause-based assessment is critical. Common causes of pleural effusion include heart failure, pneumonia, tuberculosis, pulmonary embolism, kidney disease, liver disease, autoimmune disease, chest trauma, and cancer. Causes of pleural effusion also include oesophageal rupture and lung disease. Pleural effusion risk factors, therefore, include chronic heart or kidney disease, cirrhosis, lung infections, previous cancer, smoking, thoracic surgery, chest injury, and known pleural or lung disease.

Pleural effusion treatment without surgery focuses on relieving the symptoms, treating the underlying cause, and, when possible, preventing the pleural fluid from returning.
The first step in managing pleural effusion is determining whether the excess fluid needs to be drained. A very small fluid buildup with a clear underlying cause may only need treatment of the underlying condition and monitoring. Pleural effusion treated through medical therapy alone can be effective when the cause is congestive heart failure or another systemic disease. For example, if heart failure is driving the fluid buildup, diuretics and an optimisation of cardiac care may allow the pleural fluid to settle without any procedure.
When pleural fluid is causing shortness of breath or other respiratory symptoms, or when the underlying cause needs further diagnosis, thoracentesis may be both therapeutic and diagnostic. This can improve breathing and shortness of breath while providing material for pleural fluid analysis. Pleural fluid drainage should be performed carefully to avoid reexpansion pulmonary oedema, a recognised complication when large volumes are removed too quickly.
For recurrent malignant pleural effusions, one option is pleurodesis. This aims to make the visceral pleura adhere to the chest wall, so that excess fluid has no space to reaccumulate. Another option is an indwelling pleural catheter, which allows a repeated drainage of pleural fluid at home. In infection, antibiotics are essential, but drainage is often just as important. A chest tube may be needed when pleural fluid is heavily infected, thick, or for a loculated pleural effusion. Pulmonary oedema and vascular injury are potential risks during drainage. Your healthcare provider will discuss these risks with you before any procedures.
Good pleural effusion treatment is not only about removing pleural fluid. It is about choosing the least invasive method that still effectively treats the underlying cause.

Surgery is considered when pleural effusion is complex, recurrent, infected, trapped, or associated with pleural disease requiring direct treatment.
Video-Assisted Thoracoscopic Surgery (VATS) is often the preferred minimally invasive approach when pleural effusion needs more than simple drainage. Using small incisions and a camera, the surgeon can inspect the pleural cavity, obtain biopsies, break loculations, clear infected material from the pleural space, perform pleurodesis, and release trapped lung tissue due to scarring of the chest wall. VATS is especially valuable in infected pleural conditions, recurrent undiagnosed exudative effusions, and malignant pleural disease.
At Neumark, VATS plays an important role in managing pleural effusion when the pleural fluid is complex or recurrent. It can address several problems in a single sitting, offering a major advantage over repeated blind drainage.
An open approach, though rarer, may be needed when the empyema is very advanced, when a dense pleural peel requires formal decortication, when minimally invasive access is not safe enough, or when the underlying pleural or lung disease is more extensive than expected.
Thoracotomy is more invasive, but in selected cases, it is the best route to fully clear an infection or free a lung that has become trapped against the chest wall.
The choice between VATS and thoracotomy depends on the stage of disease, the extent of pleural organisation, the patient’s overall health, and the surgeon’s judgement about which approach will most effectively resolve the problem.

Recovery after treatment for a pleural effusion depends on the underlying cause, the procedure used, and whether the lung re-expands well.
After simple thoracentesis or pleural tap, recovery is usually quick, although continuous monitoring is needed to ensure there is no bleeding, blood clot formation, infection, or procedure-related pneumothorax. After chest tube drainage, a hospital stay may be necessary because the chest tube remains in place until the pleural fluid drainage has decreased and the lung is well expanded.
After a VATS or thoracotomy, recovery takes longer but is often very worthwhile when the underlying cause is infection, trapped lung, or a recurrent symptomatic pleural fluid. Risks of intervention can include bleeding from blood vessels, chest pain, infection, an air leak, a recurrence of excess fluid, an incomplete drainage, and an injury to nearby structures. In frail patients, the underlying illness may pose a greater risk than the procedure itself.
The main pleural effusion complications come from delayed treatment or an untreated underlying disease. These include trapped lung, empyema, sepsis, persistent breathlessness, reduced lung expansion, recurrent hospital admissions, and, in malignant pleural effusion cases, repeated symptomatic fluid re-accumulation. That is why recurring or complex effusions should not be drained repeatedly without a broader plan to address the root cause.
Many patients do recover well, especially when the underlying cause is reversible, and the pleural fluid is treated early. For some, especially those with chronic heart failure or cancer, the aim is longer-term control rather than permanent cure. Even then, a thoughtful treatment plan can greatly improve comfort and function in daily life.

Neumark Lung & Chest Surgery Centre helps by identifying the underlying cause of pleural effusion, choosing the right level of intervention, and offering minimally invasive thoracic surgery when needed.
Neumark specialises in pleural and thoracic conditions with a multidisciplinary approach led by Dr Harish Mithiran, senior consultant thoracic surgeon at Gleneagles and Mount Alvernia hospitals. That means looking beyond the pleural fluid itself and focusing on the full picture: why it is there, whether it is likely to recur, whether the lung is trapped, and whether a minimally invasive surgical approach could offer a more lasting solution for patients with pleural effusion.
When simple drainage is enough, we hope to avoid unnecessary procedures. When the pleural fluid is recurrent, loculated, or suspicious for malignancy, Neumark can assess whether VATS, pleural biopsy, pleurodesis, or decortication is more appropriate.
If you have been told you have pleural effusion, or if shortness of breath, chest pain, or recurrent pleural fluid around the lung is affecting your quality of life, contact Neumark for a consultation.

