

What Is Exudative Pleural Effusion?
Exudative pleural effusion is a build-up of protein-rich fluid around the lung, usually caused by inflammation, infection, cancer, or disease affecting the pleura.
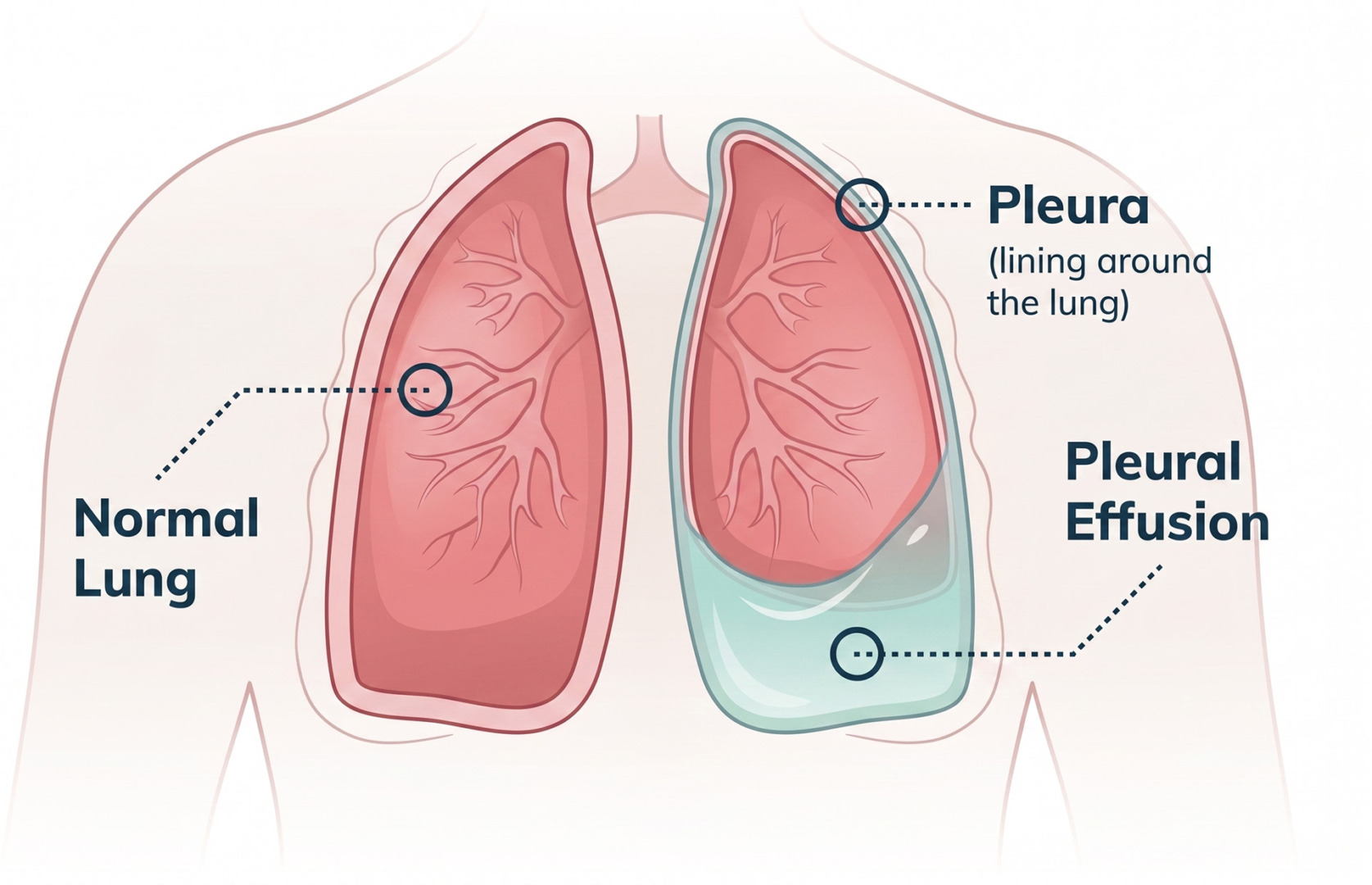
The pleura is a thin lining that covers the lungs and the inside of the chest wall. The space sits between two pleural layers: the visceral pleura, which covers the lung, and the parietal pleura, which lines the chest wall. A small amount of fluid normally sits between these layers, which helps the lungs move smoothly when you breathe. A pleural effusion happens when excess fluid collects in the pleural cavity or pleural space.
Types of Pleural Effusion
Pleural effusions are usually grouped into two main types:
- A transudative pleural effusion is usually caused by a body-wide fluid imbalance, such as heart failure, liver disease, kidney disease, nephrotic syndrome, renal failure, or peritoneal dialysis. A transudative effusion may also occur when hydrostatic pressure increases in the blood vessels or blood protein levels fall.
- An exudative pleural effusion is different. It usually means the pleura or nearby lung tissue is irritated, inflamed, infected, or affected by cancer.
This distinction matters because the treatment is different. A transudative effusion often improves when the underlying medical condition is controlled. An exudative effusion usually needs closer investigation. It may need fluid drainage, pleural biopsy, antibiotics, cancer treatment or surgery, depending on the cause.
Symptoms
Symptoms of exudative pleural effusion depend on how much fluid has accumulated and what is causing the inflammation or pleural disease.
Some people have no symptoms, especially if the effusion is small. Others develop shortness of breath, chest discomfort, dry cough, fever, tiredness, chest pain, or pain that worsens with deep breathing. The pain can feel sharp because the inflamed pleura is sensitive.
The symptoms may also point to the underlying cause.
- Fever, chills, and feeling unwell may suggest pneumonia, parapneumonic effusion, or a pleural infection.
- Weight loss, poor appetite, or recurrent fluid may raise concern for lung cancer, pleural malignancy, or a malignant pleural effusion.
- Night sweats and a prolonged cough may suggest tuberculosis or tuberculous pleurisy.
- Sudden chest pain and breathlessness may occur with pulmonary embolism.
A large effusion can press on the lung, preventing it from expanding fully. This accumulated fluid can make walking, climbing stairs, or lying flat more difficult, causing respiratory symptoms that affect daily life. If the fluid is infected or a loculated pleural effusion, divided into pockets, the symptoms may be more persistent, and the treatment may be more complex.

When to See a Thoracic Surgeon
You should see a thoracic surgeon when pleural fluid is unexplained, recurrent, infected, complex, or suspicious for cancer. Not every pleural effusion needs surgery. However, exudative effusions often need more detailed evaluation because they may be linked to an infection, malignancy, pulmonary embolism, rheumatoid arthritis, autoimmune disease, or other pleural disorders.
A thoracic surgeon is especially important when the fluid keeps returning, drainage is incomplete, the lung is trapped, or tissue is needed for diagnosis. Specialist review is also important if the effusion is associated with pleural thickening, pleural nodules, pus, blood-stained fluid, or a lung mass seen on a CT scan.
You should seek urgent medical attention if you have severe breathlessness, chest pain, high fever, confusion, blue lips, or rapidly worsening symptoms. These may suggest a serious infection, large effusion, pulmonary embolism, or another chest emergency.

Diagnosis
The diagnosis of exudative pleural effusion begins with imaging and is confirmed by pleural fluid testing.
A chest X-ray may show fluid at the base of the lung. It can also help determine whether the effusion is small, large, or mainly unilateral. Ultrasound scans can detect smaller collections and help guide safe drainage. A CT scan provides greater detail and can show pleural thickening, lung infection, tumours, lymph nodes, loculated fluid, or a trapped lung.
Thoracentesis is often the key test. During this procedure, a needle is used to remove a fluid sample from around the lung. The sample is sent to the lab to help determine whether the fluid is transudative or exudative and to look for infection, cancer cells, blood, or other clues to the pleural effusion.
Doctors may take a small sample of fluid from around the lung and send it to the lab. This helps them understand why the fluid has built up. The lab checks the fluid for protein and sugar levels, cell counts, signs of infection, and the presence of cancer cells. It may also check a substance called LDH, which can rise with inflammation, infection, tissue irritation, or cancer.
Doctors compare the results from the lung fluid with the results from the blood. If the fluid has higher-than-expected protein or LDH levels, it is more likely to be an exudative pleural effusion. This means the fluid is probably due to a problem affecting the lung lining, such as an infection, inflammation, cancer, or another pleural disease. A low pleural fluid pH may suggest a complicated parapneumonic effusion. Pleural fluid pH and pleural pH can help decide whether chest tube drainage is needed.

Non-Surgical Management of Pleural Effusion
The non-surgical treatment for exudative pleural effusion focuses on draining the pleural fluid when needed and treating the underlying cause.
If the effusion is small and symptoms are mild, doctors may monitor it while treating the cause. For example, pneumonia-related fluid may improve with antibiotics. A parapneumonic effusion may require closer monitoring if a fever, elevated infection markers, or a pleural fluid pH test suggests a complicated parapneumonic effusion. Inflammatory causes may need treatment for the underlying autoimmune condition, such as rheumatoid arthritis. A pulmonary embolism requires blood-thinning treatment unless there is a reason not to use it.
When the fluid causes breathlessness or when the diagnosis is unclear, thoracentesis can relieve symptoms and provide fluid for testing. Some patients need a chest tube if the fluid is large, infected, thick, or difficult to drain with a single needle procedure.
In a pleural infection, antibiotics are essential, but drainage is often just as important. If infected fluid becomes thick or forms pockets, medication may be administered through the chest tube to help break up the loculations. If this does not work, surgery may be needed.
For a malignant pleural effusion, the treatment will depend on the cancer type and the person’s overall condition. Options for a malignant pleural effusion may include repeated drainage, an indwelling pleural catheter, pleurodesis, chemotherapy, immunotherapy, targeted therapy, or palliative treatment focused on breathing comfort and quality of life.
Surgical Options
Surgery is considered when exudative pleural effusion is recurrent, infected, loculated, difficult to diagnose, or causing a trapped lung.
- Video-Assisted Thoracoscopic Surgery (VATS) is often the preferred surgical approach. It uses small incisions and a camera to look inside the chest. Through VATS, the surgeon can drain accumulated fluid, inspect the pleural cavity, break down pockets of infection, remove infected material, take pleural biopsies, perform pleurodesis, or free a trapped lung by removing thick fibrous tissue called a pleural peel. VATS is especially useful when pleural infection has not improved with antibiotics and chest tube drainage. It is also helpful when lung cancer, pleural malignancy, or malignant pleural effusion is suspected, but fluid tests have not given a clear diagnosis. Direct visualisation of the pleura and targeted biopsies can improve diagnostic accuracy.
- Thoracotomy is an open chest operation. It is used less often because it is more invasive. It may be needed when the infection is advanced, the pleural peel is very thick, the lung is severely trapped, or minimally invasive surgery is not safe or complete enough.
The choice between VATS and a thoracotomy depends on the cause, the stage of pleural disease, the patient’s fitness, and whether the goal is diagnosis, drainage, infection control, or recurrence prevention.

Risks and Recovery
The recovery after treatment for exudative pleural effusion depends on the cause, the procedure used, and how well the lung re-expands.
- After a thoracentesis, many patients feel relief from being able to breathe quickly. Possible risks include pain, bleeding, infection, and a pneumothorax, which is air leaking into the space around the lung. These complications are uncommon when the procedure is carefully guided, but monitoring remains important.
- After chest tube drainage, patients with infection may need several days in the hospital for antibiotics, drainage and repeat imaging.
- After VATS, recovery is usually faster than after a thoracotomy. Patients are encouraged to walk early, do breathing exercises, and use pain medicine so they can cough and breathe deeply. A chest drain may remain for a short time. A thoracotomy usually involves a longer hospital stay and slower recovery because the incision is larger.
Recurrence depends on the underlying cause. Pneumonia-related effusions may resolve fully. Malignant effusions may come back unless pleurodesis, an indwelling catheter, or cancer treatment controls the fluid.
How Neumark Can Help
Neumark Lung & Chest Surgery Centre helps identify the cause of exudative pleural effusion and provides appropriate treatment, ranging from drainage to minimally invasive surgery.
Neumark specialises in pleural and thoracic conditions with a multidisciplinary approach led by Dr Harish Mithiran, senior consultant thoracic surgeon at Gleneagles and Mount Alvernia hospitals. For patients with exudative pleural effusion, this means carefully reviewing imaging, fluid results, symptoms, and overall health before recommending treatment.
Some patients need only targeted medical treatment and monitoring. Others need thoracentesis, chest tube drainage, VATS pleural biopsy, pleurodesis, or decortication. When surgery is appropriate, Dr Harish may use minimally invasive thoracic surgery techniques to treat pleural disease while reducing surgical trauma where possible.
If you have been told you have an exudative pleural effusion, or if fluid around the lung keeps returning, contact Neumark for a consultation.