

What Is Pectus Excavatum in Women?
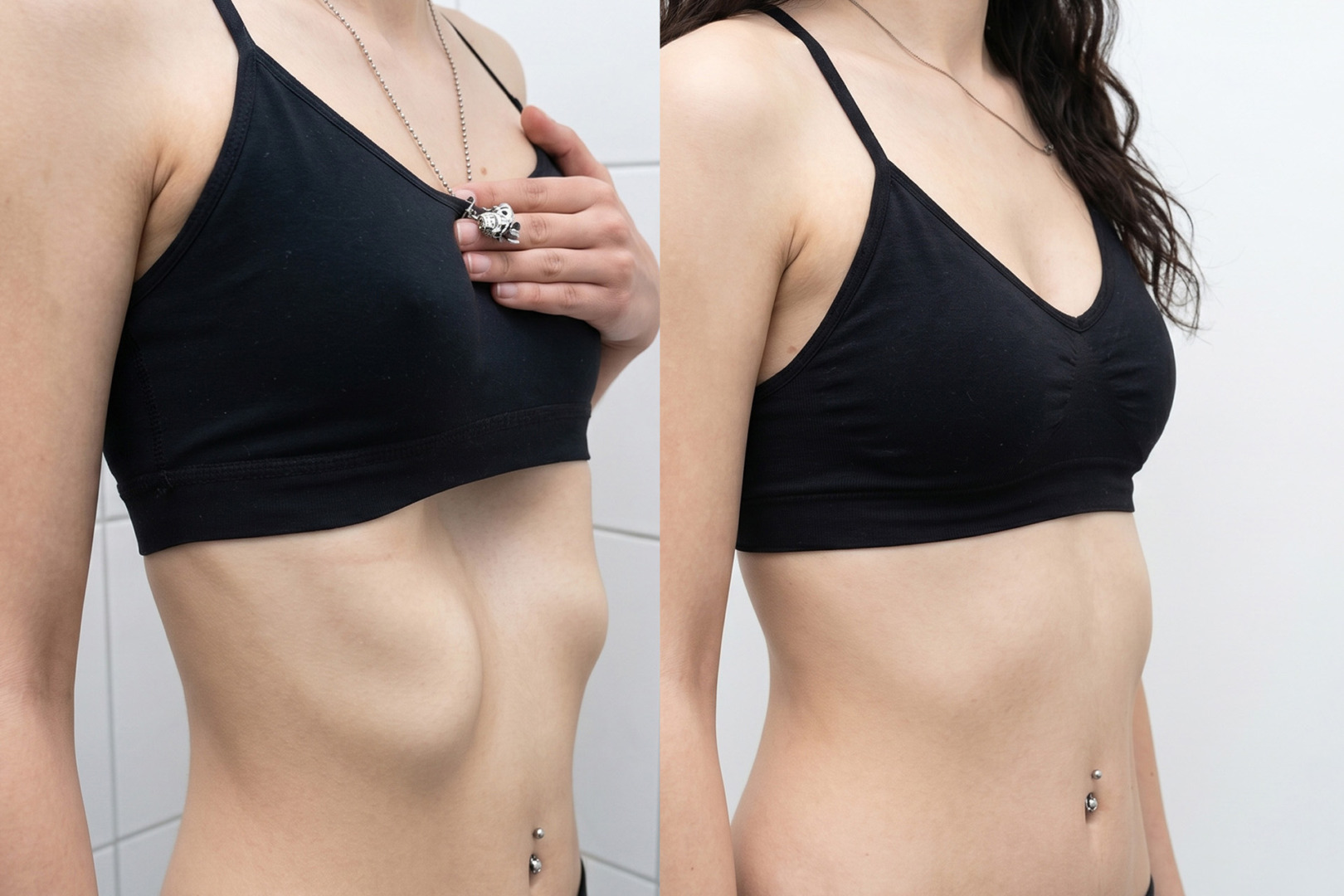
Pectus excavatum in women is a chest wall condition in which the breastbone sinks inward, creating a hollow or sunken appearance of the chest.
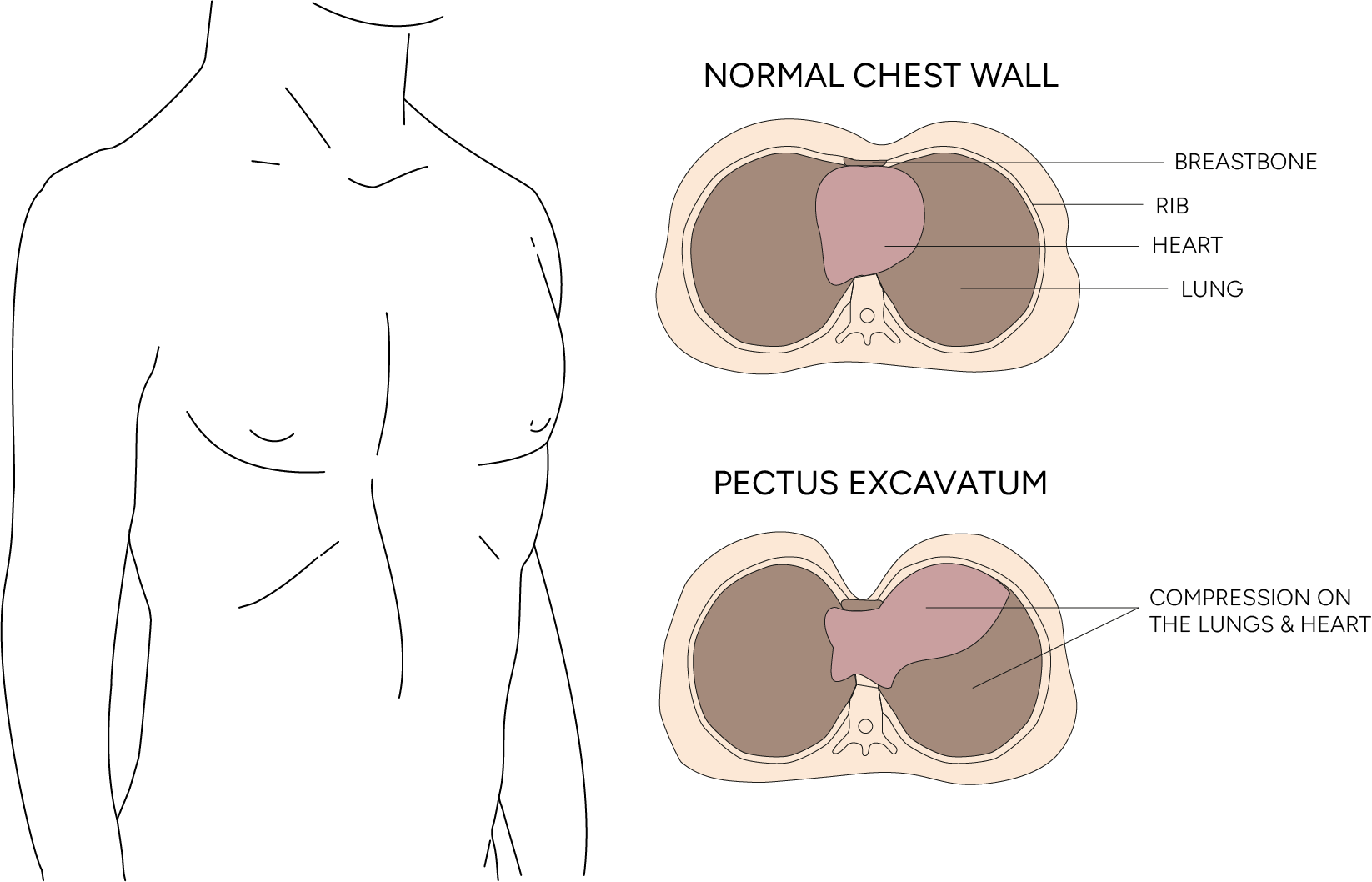
Pectus excavatum is sometimes called funnel chest. As a congenital chest wall deformity, this funnel chest shape is present from birth. A related congenital condition, pectus carinatum, pushes the breastbone outward instead. Pectus carinatum and excavatum are opposite patterns within the same family of chest wall deformities. It happens when the sternum, the breastbone, and nearby ribs grow inward rather than forming a flat front. The depth and shape of the sunken breastbone can vary. Some women have a mild indentation. Others have a deeper or uneven depression that affects posture, breathing, exercise tolerance, and body confidence.
Pectus excavatum occurs in about 1 in 300 to 1 in 1,000 births. It is more common in males, with an approximate male-to-female ratio of 3:1.
Women may notice that the hollow sits between the breasts, affects the way the breasts appear, or makes one side look different from the other. Some may feel that the breasts look widely spaced, uneven, or pulled inward by the depression itself.
Pectus excavatum is often hereditary and can run in families. It may also be associated with a connective tissue disorder, such as Marfan syndrome, Ehlers-Danlos syndrome, or, less often, osteogenesis imperfecta, each of which affects the bones and joints. Other genetic risk factors include Noonan syndrome and Turner syndrome. These conditions can affect the bones, joints, skin, and other tissues.
Pectus excavatum may be present from early childhood. A child’s chest may look only slightly hollow, but the deformity often becomes more noticeable during puberty and the adolescent growth spurt, when the sternum and breast tissue develop. In older children, young adults, and women, a second growth spurt-like change in chest shape is uncommon, but the indentation may appear deeper.
Symptoms of Pectus Excavatum
Symptoms of pectus excavatum in women may include sternal changes, breathing difficulty, exercise limitation, chest pain, and concerns about appearance.
Many women have mild pectus excavatum and no physical symptoms. Others may notice shortness of breath during exercise, reduced stamina, discomfort, back pain, heart palpitations, or a feeling of pressure across the front. Symptoms can be more noticeable during sport, climbing stairs, or other activities that increase breathing demand.
Some women also describe poor posture, rounded shoulders, or a tightness across the front. These changes can develop as the body adapts to the sunken chest shape.
Women with pectus excavatum may present with more severe chest wall deformities than men, which can be uneven or deeper on one side. The hollow may affect how clothing fits, how the breasts appear in clothing, or how comfortable a woman feels in swimwear, sportswear, or fitted tops. For some women, the emotional impact is as significant as the physical symptoms.
Women with pectus excavatum may also have higher preoperative pain profiles, meaning they may report more pain before surgery than expected from the visible shape alone.
Pectus excavatum does not usually prevent pregnancy or breastfeeding. Most women with mild or asymptomatic pectus excavatum can have normal pregnancies. Severe pectus excavatum, with a deep dent in the chest and severe symptoms, is uncommon, but in severe cases, the deformity affects breathing or pulmonary function. Specialist review before pregnancy or major surgery planning may be helpful, and treatment can improve symptoms in selected severe cases.

When to See a Thoracic Surgeon
You should see a thoracic specialist if pectus excavatum causes symptoms, appears to be worsening, affects confidence, or raises concern about heart or lung compression.
Specialist review is especially important if you have shortness of breath, chest pain, reduced exercise tolerance, palpitations, dizziness, repeated lower respiratory infections, or a deep indentation that appears to be worsening. It is also sensible to seek an assessment if the condition is causing distress about your breast symmetry and appearance.
A thoracic surgeon can help determine whether the condition is mainly cosmetic, functional, or both. This distinction matters because the treatment should match the problem. Some women need reassurance and monitoring. Some benefit from physiotherapy and posture work. Others may need further testing to see whether the sunken sternum is pressing on the heart or lungs.
Diagnosis of Pectus Excavatum
Pectus excavatum in women is primarily diagnosed through a physical examination, and the appropriate treatment follows from that assessment.
A chest X-ray or CT scan may be used to assess the sternum and ribs and to measure the severity of the condition. A CT scan can show how much the breastbone is depressed, the position of the lower breastbone, and whether the heart and lungs are being compressed. One commonly used measurement is the Haller index, which compares chest width to the distance between the breastbone and the spine. A normal Haller index is usually 2.5 or less. A Haller index greater than 3.25 generally indicates significant pectus excavatum and is one factor used when considering surgery.
Other tests may be needed if the symptoms suggest the heart and lungs are involved. These can include pulmonary function tests, an electrocardiogram, an echocardiogram, or exercise testing of the heart and lungs. These tests help show whether breathlessness or reduced stamina is due to the pectus excavatum, deconditioning, asthma, heart rhythm problems, or another condition.
In women, the assessment should also consider the asymmetry of the sternum and the breast appearance. Pectus excavatum can make the breasts appear uneven, even when the breast tissue itself is normal. A clear diagnosis helps separate sternum shape from breast disease or other causes of asymmetry.

Non-Surgical Management of Pectus Excavatum
Non-surgical management may help women with mild pectus excavatum, especially when the symptoms are limited and there is no significant compression of the heart or lungs.
For mild cases, an observation may be enough. Regular reviews can track whether the deformity is stable or changing. Physiotherapy may help improve posture, shoulder position, chest wall mobility, and breathing mechanics. These measures do not usually correct the bone shape, but they may improve the comfort, appearance, and exercise confidence.
Breathing exercises and general fitness training can help some women feel more in control of their symptoms. If the pain is related to muscle tightness or posture, targeted physiotherapy may reduce the strain. Psychological support can also be valuable when body image concerns are affecting confidence or daily life.
The vacuum bell is a medical device used as a non-surgical treatment for selected patients with mild or flexible pectus excavatum. It uses suction to gently lift the sunken sternum over time. It is not suitable for everyone, and results may vary; it tends to be more effective in younger patients with more flexible chest walls.
Breast implants or fat transfer may improve selected cosmetic concerns, but they do not correct the underlying chest wall depression. Customised 3D silicone implants can also be used in selected cases to improve the contour. These implants may help camouflage the hollow, but they do not move the breastbone or treat heart or lung compression.
In women with a deeper central hollow, treating breast shape alone may not address the main structural issue. A thoracic assessment can help clarify which concern should be treated first.
Surgical Options for Pectus Excavatum
Surgery may be considered when the pectus excavatum is moderate to severe, causes symptoms, affects heart or lung function, or has a major impact on the patient’s quality of life.
Surgery is often recommended when the Haller index is greater than 3.25, especially when this is combined with symptoms, heart or lung compression, or significant quality-of-life impact. Treatment for pectus excavatum is not based on one number alone. Imaging, physical symptoms, exercise capacity, pain, psychological impact, and patient goals all need to be considered.
Surgical treatment to correct pectus excavatum involves one of two traditional operations:
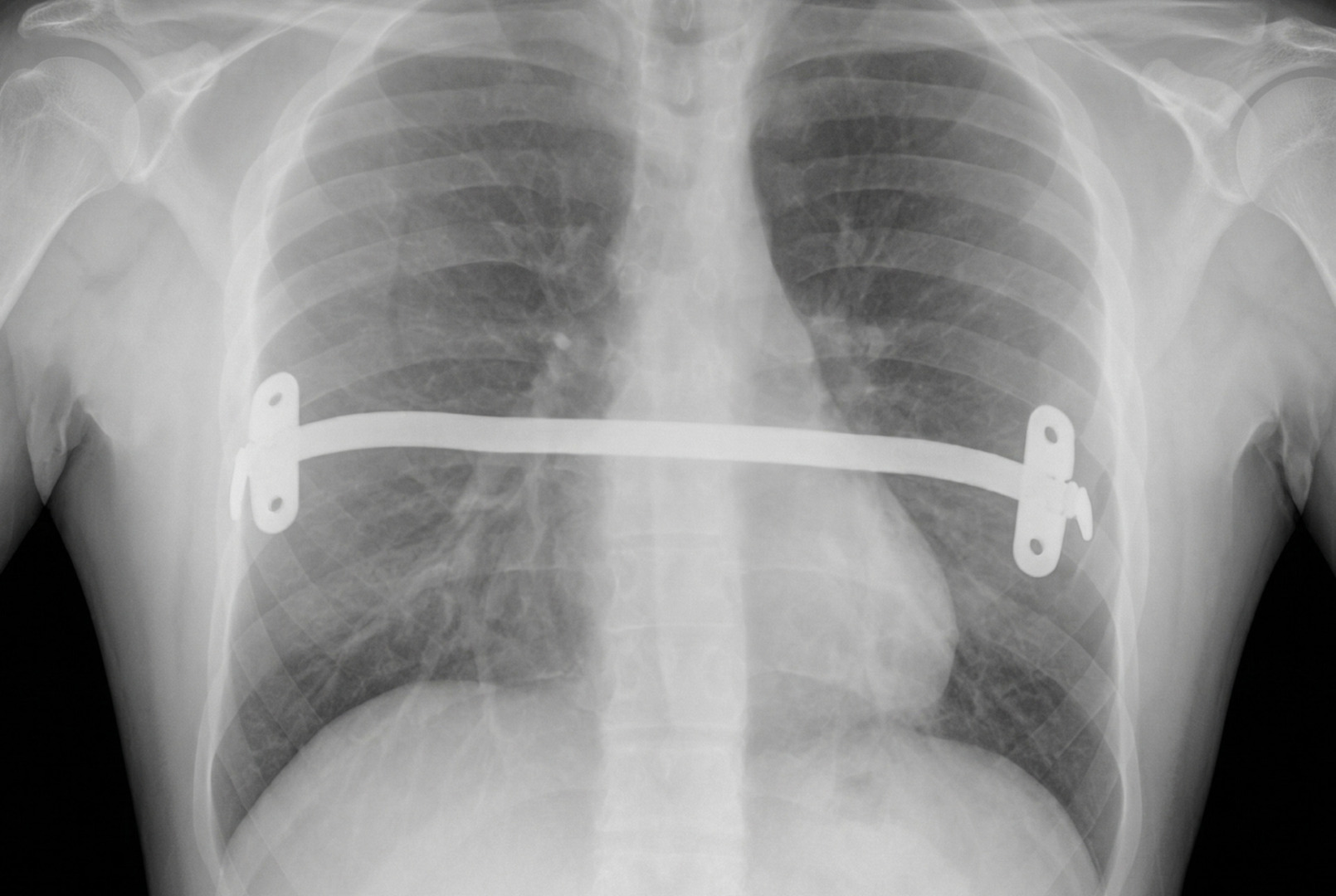
- The Nuss procedure uses only small incisions. The surgeon makes small incisions on each side of the chest and, through those small incisions, places a curved metal bar under the breastbone. The metal bar is shaped to fit the chest. The bar lifts the breastbone forward into a more normal position. In wider or asymmetric cases, more than one bar may be used to spread the lifting force. As a minimally invasive correction, the Nuss procedure typically takes 1 to 2 hours under general anaesthesia, with a short hospital stay for most patients. The bars are usually removed after 2 to 3 years, although surgical hardware may be removed after 1 to 2 years in selected cases, depending on the technique, age, healing, and the surgeon’s recommendation.
- The Ravitch procedure is an open repair. This surgical repair involves removing or reshaping deformed costal cartilage and repositioning the breastbone, lifting the lower breastbone into a better position. Although it is an open repair, careful technique limits scarring. It may be considered for more complex, rigid, or asymmetric deformities, especially in adults.
{kind=link}
Surgery is not suitable for every woman with pectus excavatum. Surgical planning needs careful attention to breast position, incision placement, symmetry, and the shape of the central chest. A good result should address function where needed while also respecting cosmetic concerns. In some cases, staged treatment may be discussed if breast asymmetry remains after sternal correction.
Cost of Surgery for Pectus Excavatum
For women, the cost of pectus excavatum surgery in Singapore depends on the type of correction needed, the severity and symmetry of the chest wall deformity, the length of hospital stay, the surgeon’s fees, and whether surgical bars or implants are used.
Some women may also need treatment planning that considers breast position, chest contour, scarring, and whether the main goal is functional improvement, cosmetic correction, or both. Many insurance plans may cover medically necessary chest wall surgery, but coverage varies by policy and often requires pre-authorisation, imaging results, and supporting clinical documentation.
Your thoracic surgery team can provide a detailed estimate during the consultation and advise you on the paperwork your insurer may need.
Risks and Recovery
Recovery after pectus excavatum surgery depends on the type of surgery, age, chest wall stiffness and overall health.
After surgery, pain management is important because the sternum has been repositioned. Patients are encouraged to breathe deeply, walk early, and follow activity restrictions while it heals. Heavy lifting, contact sports, and intense upper-body physical activity are usually avoided for a period of time, and patients return to lighter physical activity in stages.
Possible risks include bleeding, infection, bar movement, pneumothorax, fluid around the lung, pain, recurrence, scarring, and the need for further surgery. In women, there may also be concerns about visible scars, breast contour, or persistent asymmetry. These should be discussed before the operation to ensure expectations are realistic.
Most patients recover gradually. The visible shape may improve soon after surgery, but full healing takes longer. If a bar is placed, a second procedure is usually needed later to remove it. Long-term results are often good in carefully selected patients.
How Neumark Can Help
Neumark Lung & Chest Surgery Centre helps women with pectus excavatum understand whether their condition needs monitoring, non-surgical care, or thoracic surgery.
Neumark specialises in minimally invasive thoracic surgery with a multidisciplinary approach led by Dr Harish Mithiran, senior consultant thoracic surgeon at Gleneagles and Mount Alvernia hospitals.
If you are a woman with pectus excavatum, or if you are worried about a sunken chest, breast asymmetry, breathlessness, exercise limitation, or chest discomfort, contact Neumark for a consultation to discuss your treatment options.