

Benign nodules and benign conditions are the most common causes of lung lesions. They may be due to granulomas, hamartomas, chronic inflammation from granulomatous diseases such as rheumatoid arthritis, or scar tissue. Malignant nodules include primary lung cancers, such as small cell lung cancer, and metastases from cancers elsewhere in the body. A malignant nodule may need further evaluation to determine the best treatment.
Risk factors such as smoking (in former smoker patients too), age, family history and exposure to asbestos or air pollution influence how likely a lesion or nodule is to be cancerous. It is important to distinguish lung lesions from other diseases with similar imaging features through differential diagnoses, which may sometimes necessitate a biopsy. Chronic obstructive pulmonary disease can also present with lung abnormalities.
If you are asking what the common symptoms of lung lesions are, the honest answer is that they are often non-specific, which is why imaging tests and clinical review are so necessary. Many do not cause any symptoms. Notably, the absence of symptoms does not rule out a significant finding. When symptoms do occur, they may include a persistent cough, shortness of breath, chest pain or chest discomfort, coughing up blood, wheezing or unexplained weight loss.

The first step after finding a lesion on a lung CT scan is to review the images in detail. A chest X-ray can offer some clues, but a chest CT will provide accurate information about size, shape, density, and location. Chest CT scans are a crucial imaging test for identifying and characterising pulmonary nodules and pulmonary lesions. Radiologists look for features such as smooth or spiculated margins, calcification patterns (e.g., calcium deposits or calcified lung nodules), growth over time, and whether the nodule is solid, subsolid, or ground-glass in appearance. These CT findings are essential for your specialist to estimate the risk.
A PET scan may be performed after a chest CT to further evaluate the findings. If you are wondering what percentage of pulmonary nodules are likely to be cancerous, there is no definitive answer, as it depends on the size, appearance, and risk profile. In lung cancer screening and in the general population, most incidental pulmonary nodules are benign. Even so, caution is warranted because early detection of lung cancer is difficult, and lung nodules rarely show symptoms initially.

A lung lesion biopsy is often the key to the final diagnosis, and the method is determined by the lesion’s location in the lung parenchyma. Peripheral lesions are usually sampled with CT-guided needle biopsy, while central or airway-adjacent lesions can be reached via bronchoscopy. In some cases, a minor surgical biopsy is the safest option for obtaining sufficient tissue for accurate analysis. Pathology confirms whether the lung lesion is benign or malignant and, if lung cancer, identifies the type.
Only a biopsy can provide a definitive diagnosis of whether a lung lesion is cancerous, as imaging tests alone cannot confirm malignancy. Molecular testing can reveal mutations that guide targeted therapies. A timely lung cancer diagnosis is crucial for improving lung cancer survival rates, reducing patient anxiety, and enabling early detection.

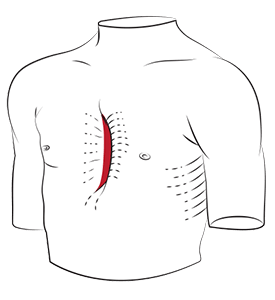
If a lung lesion or mass is likely malignant, growing, or causing symptoms, removal may be advised. At Neumark Lung and Chest Surgery Centre, we use minimally invasive techniques for thoracic surgery wherever safe and appropriate.
Video-Assisted Thoracoscopic Surgery (VATS) uses small incisions and a camera to access the chest. Uniportal VATS achieves this through a single incision. Robotic-Assisted Thoracic Surgery (RATS) adds three-dimensional vision and wristed instruments for precise dissection in tight spaces. These approaches allow wedge resection for diagnosis, segmentectomy to remove a segment, or lobectomy when a larger portion is needed in the right lung or upper lobe. Lymph nodes are sampled to stage lung cancer accurately. Patients usually experience less pain and a faster recovery compared to traditional open surgery. Radiation therapy may be considered for patients who are not surgical candidates.
For benign tumours that are growing or causing symptoms, minimally invasive resection is also often the best solution. It confirms the nature of the pulmonary lesions and prevents future complications.

If lung lesions are left unmonitored or untreated, they can sometimes lead to serious complications. Malignant lesions may progress to lung cancer, which can spread to other parts of the body and become life-threatening. Other risks include respiratory failure or persistent symptoms such as chest pain, shortness of breath or unexplained weight loss.
If you have a medical history of lung cancer or other lung diseases, you should be more proactive about regular screenings as a screening test and follow-up. Early medical attention and timely treatment are the best ways to minimise the risks of lung nodules.
When surgery is not advised due to other health conditions after a physical examination, alternatives may include stereotactic body radiotherapy, which delivers focused radiation to a small area, or thermal ablation techniques such as radiofrequency ablation. These methods can control selected larger nodules and are considered on a case-by-case basis after multidisciplinary review. Internal medicine specialists are often involved in evaluating complex cases where surgery is not suitable.

Finding a lesion on a lung CT scan or computed tomography (CT) scan or computed tomography ct does not mean you have lung cancer. Your clinical team will review the features of the nodule, your high-risk factors, and your overall health to assess your situation. They will advise whether monitoring, needle biopsy or removal is best. If surgery is needed, minimally invasive techniques mean most patients recover quickly, often leaving the hospital in a few days.
At Neumark, we focus on accuracy, clear communication, and tailored care. Our team has broad experience in managing lung lesions and pulmonary nodules, from surveillance plans to complex resections using VATS, U-VATS and robotic approaches.
If you have concerns about a lung lesion or lung nodules or want a second opinion, contact Neumark Lung & Chest Surgery Centre. We consult and operate at Gleneagles Hospital and Mount Alvernia Hospital, with full support from the imaging, respiratory, and oncology teams. Call +65 6908 2145 or WhatsApp +65 9726 2485 to book a consultation. Early, expert care matters for lung lesions and lung nodules, whether in a former smoker or as an incidental finding, the size of a green pea.