

In many patients, metastatic lung cancer symptoms are mild or even absent in the early stages, which makes detection difficult. Additionally, the symptoms of metastatic lung cancer can vary depending on the location and extent of metastasis, but there are some key signs to look out for:
As these symptoms overlap with those of other respiratory conditions, they are often overlooked. If you have a history of cancer and develop new or unexplained chest symptoms, seek medical evaluation promptly.

Treatment for metastatic lung cancer depends on the primary cancer type, how far it has spread, and the patient’s overall health. Systemic therapies, such as chemotherapy, targeted drugs, and immunotherapy, form the foundation for controlling tumour growth and improving survival. These treatments can have side effects that affect a patient’s quality of life. It is important to discuss potential side effects and their management with your healthcare team.
Radiation therapy, including advanced techniques like stereotactic body radiotherapy (SBRT), is often used to relieve symptoms like chest pain or breathing difficulties and to control small, well-defined lesions. In selected cases, surgery for metastatic lung cancer, known as pulmonary metastasectomy, can remove lung nodules to relieve symptoms and extend life expectancy.
Lung cancer surgery is usually considered when the primary cancer is controlled, no disease is present outside the lungs, and lung function is strong enough to support recovery. It is very rarely an option when the source of the cancer has not undergone treatment.
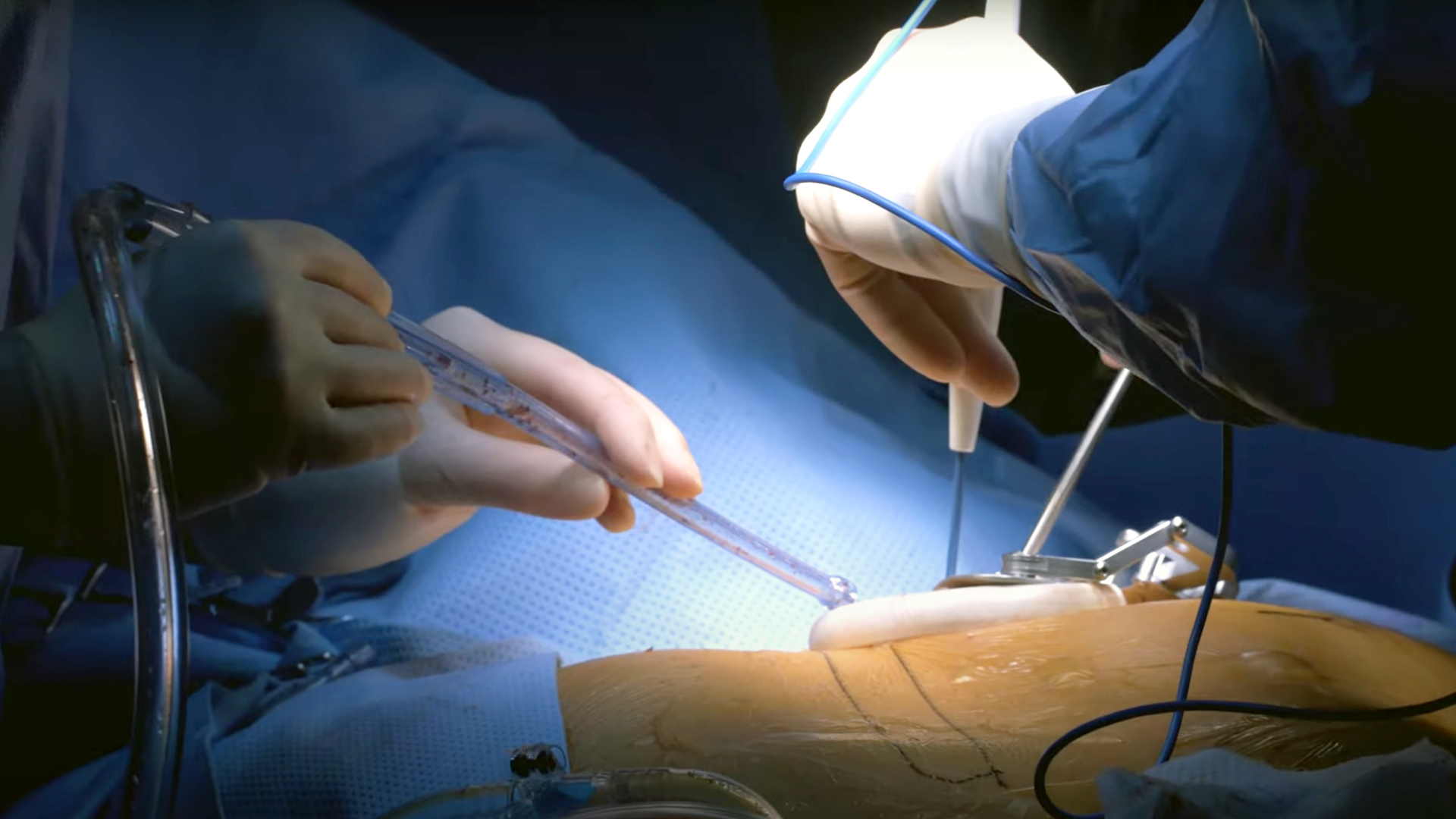
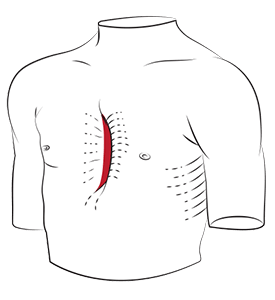
Video-Assisted Thoracic Surgery (VATS), commonly known as VATS, is a game-changing approach in treating metastatic lung cancer, utilising small incisions and a camera-guided system to remove lung tissue. This minimally invasive technique offers several advantages over open surgery, including reduced postoperative pain, a shorter hospital stay, and a faster recovery time, allowing patients to return to their daily lives sooner.
VATS is particularly well-suited for resecting solitary or limited metastatic lesions, especially those located peripherally near the lung’s surface. It excels in procedures like wedge resections or segmentectomies, which target metastatic nodules while preserving as much healthy lung tissue as possible, an important consideration for patients with metastatic lung cancer who may face multiple interventions due to recurrent disease.
The magnified, high-definition views provided by VATS allow surgeons to identify and excise lesions with precision, minimising trauma to surrounding tissues. However, its effectiveness is not uniform across cases; for example, it decreases in centrally located metastases or in complex cases that require extensive lymph node dissection or intricate reconstructions, such as sleeve lobectomies. Additionally, VATS can be challenging when multiple metastases are scattered across different lung lobes or when adhesions from prior surgeries complicate access.
For patients with good lung function and limited disease burden, VATS is often the preferred option, especially when rapid recovery is a priority, such as in those undergoing staged resections for metastatic disease.

Robotic-Assisted Thoracic Surgery, or RATS, utilises advanced robotic technology to deliver unparalleled precision, dexterity, and 3D visualisation, enabling surgeons to tackle complex metastatic lung cancer cases with great accuracy, even in confined anatomical spaces. This is particularly useful for challenging cases, such as metastases near critical structures, such as major blood vessels or airways, or when a lobectomy is required for larger or centrally located lesions.
The 3D visuals allow surgeons to pinpoint small or deeply embedded metastases, while its articulated instruments provide access to hard-to-reach areas. Its tremor-free precision is particularly valuable for preserving lung function, a critical consideration for individuals with compromised respiratory capacity or a history of thoracic surgery, where adhesions may complicate access.
For simpler procedures, such as wedge resections of peripheral metastases, the benefits of RATS may not be necessary. However, RATS is often the preferred choice for complex metastatic lung cancer cases, offering a tailored solution that balances oncologic efficacy with the goal of maintaining quality of life through precise, minimally invasive intervention.

Several factors influence whether VATS or RATS is chosen for surgery for metastatic lung cancer:
At Neumark, we work with each patient to weigh these factors and design an approach that balances effectiveness and recovery.

Metastatic lung cancer prognosis for patients with metastatic lung cancer depends on several important factors, including the type of lung cancer, how far it has spread, the patient’s overall health, and how well the cancer responds to treatment. Metastatic lung cancer has a lower 5-year survival rate, roughly ranging from 3% to 9% for those with distant metastases. However, every patient is unique, and advances in lung cancer treatment have helped some patients live longer and have a better quality of life.
Patients with metastatic lung cancer are encouraged to have an open discussion with their doctor about their individual prognosis and what to expect from treatment. Understanding the likely course of the disease can help patients and their families make informed decisions about their care, set realistic goals, and focus on what matters most to them during treatment.

Metastatic lung cancer is a complex condition, but with early diagnosis, personalised treatment, and access to the latest surgical techniques, patients can see significant improvement in both longevity and quality of life.
At Neumark Lung & Chest Surgery Centre, our expertise in VATS and RATS, combined with a multidisciplinary approach, means each patient receives individualised care. We perform all surgical procedures at our affiliated institutions, Gleneagles Hospital and Mount Alvernia Hospital, ensuring access to full inpatient and critical care support.
If you or a loved one has been diagnosed with metastatic lung cancer, contact Neumark Lung Cancer Treatment Centre today. Our team will guide you through diagnosis, treatment, and recovery with care and expertise.