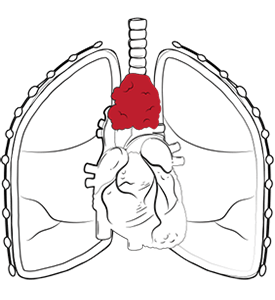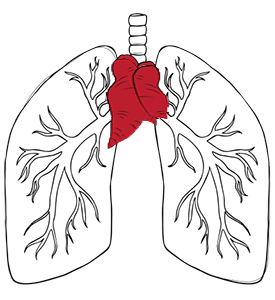


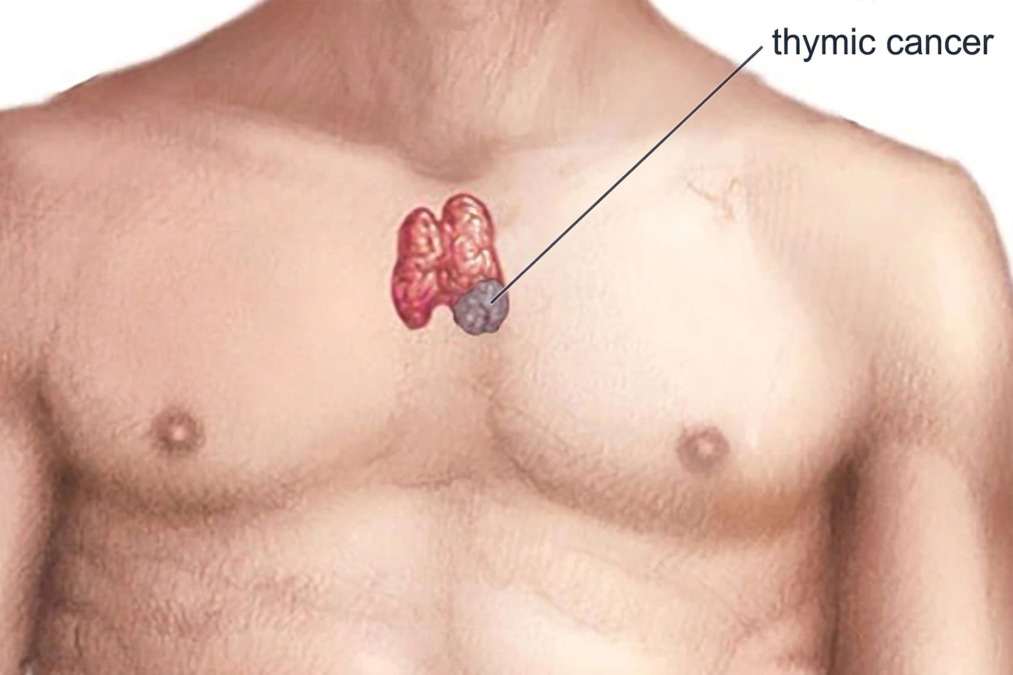
Thymic cancer or thymus cancer is a rare cancer that starts in the thymus gland, a small organ in the front of the chest cavity that sits behind the breastbone and above the heart, between the lungs.
The thymus gland helps the immune system develop early in life, especially by supporting the maturation of T lymphocytes (white blood cells). In adults, the thymus gland becomes less active, but it can still develop thymus tumours.
This is a rare cancer diagnosis, but it is important because thymus cancer treatment and management depend heavily on the exact tumour type and stage. Surgery remains the main cancer treatment whenever full removal is feasible, while chemotherapy, radiation therapy and other systemic treatments are used when the disease is advanced thymus cancer or a recurrent condition.
The broad goal is to determine whether the entire tumour can be removed, whether cancer treatment is needed before or after surgery, and whether associated immune system problems are present.
Thymic cancer is a cancer that develops from epithelial cells on the outer surface of the thymus gland. The tumour cells replace normal cells, forming a mass.
Types of thymus cancer include thymoma and thymic carcinoma. These tumours usually arise in the anterior mediastinum, the chest cavity just behind the breastbone. They differ from other masses, such as lymphoma, germ cell tumours, thymic cysts, and thymic hyperplasia.
Little is known about why thymus tumours develop, making answering the question of how someone gets thymus cancer very difficult to answer.
Types of thymus tumours include thymoma and thymic carcinoma, which differ in specific ways.
Thymus cancer symptoms are often absent in the early stages. In some cases, the mass is incidentally detected on a chest X-ray or CT scan without any symptoms.
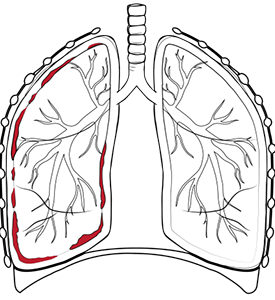
Local symptoms of thymus cancer tend to appear when the tumour presses on nearby organs and blood vessels. These can include:
As the thymus gland lies close to major blood vessels, some tumours can cause superior vena cava syndrome, leading to swelling of the face, neck, upper body or arms.
Symptoms can also arise from autoimmune diseases rather than from chest pressure. In thymoma and thymic carcinoma, myasthenia gravis may cause drooping eyelids, double vision, muscle weakness, fatigue, shortness of breath, and difficulty swallowing.

Thymus cancer diagnosed early with imaging tests has a better prognosis for the patient. There is no routine population screening programme for thymic cancer. If you are wondering how to detect thymic cancer, it is usually discovered after a chest X-ray or CT scan. A CT scan is usually the key imaging test because it shows the size of the mass, whether the cancer has spread, whether it is invading nearby structures, and whether there are suspicious lymph nodes or pleural deposits.
Magnetic resonance imaging (MRI) can provide additional detail in selected cases, especially when there is concern about pericardial or great-vessel involvement. PET-CT scans may help assess disease extent. Blood tests and lung function tests may also be part of the work-up. A thorough physical examination of the chest and neck is important.
If scans strongly suggest a resectable thymoma and surgery is already the preferred treatment, some teams may proceed directly to operation. A biopsy becomes more important when the cancer diagnosis is unclear, when the lymphoma or germ cell tumour is a possibility, or when there is suspicion of a thymic carcinoma or an unresectable disease.

Staging describes whether the thymic cancer is confined to the thymus or has spread into nearby structures or distant sites:
Thymus cancer survival rate depends on whether the tumour is a thymoma or a thymic carcinoma, how far it has spread, and whether it can be completely removed. Data from the American Cancer Society for thymus cancer show overall a 5-year relative survival of 94% for localised disease, 79% for regional disease, and 42% for distant disease. These figures are useful for context, but they are group estimates, not individual predictions.
Non-surgical cancer treatment is important when surgery is not possible or is not enough on its own.
Chemotherapy and radiation therapy are the main non-surgical treatments for thymic epithelial tumours. Common chemotherapy drugs used to treat cancer include cisplatin-based regimens that destroy cancer cells and kill cancer cells in the thymus gland. Radiation therapy may also be used to destroy cancer cells.
Anti-cancer treatments may be used before surgery to shrink a tumour that is close to being resectable, after surgery to lower the risk of recurrence, or as primary treatment when complete removal is not possible. For thymic carcinoma treatment, chemotherapy alone or chemotherapy with radiation therapy is often used.
When patients ask how to prevent thymus cancer, the most accurate answer is that there is no proven strategy. In practical terms, the most helpful step is the timely evaluation of an unexpected mediastinal mass or unexplained symptoms.
Thymus gland cancer treatment options include surgery alone or surgery combined with other therapies. However, surgery is the main treatment when the tumour can be removed completely.
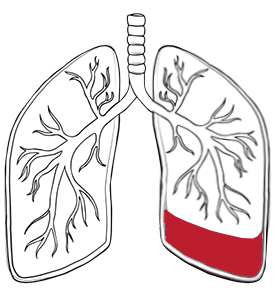
The standard operation is a thymectomy, which removes the thymus gland and the entire tumour along with any cancerous cells. Depending on the case, nearby fat, lymph nodes, pleura, pericardium or nearby organs, including a small part of the lung, may also need to be removed for a complete resection. Normal cells surrounding the tumour are preserved whenever possible.
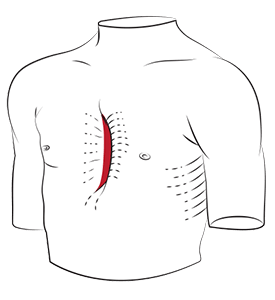
When patients ask how to remove thymus cancer, the answer depends on the tumour size, invasion and the location. Some operations require an open sternotomy for safe access, especially for large or invasive tumours. Others can be performed through minimally invasive approaches in certain cases.
At Neumark Lung & Chest Surgery Centre, Dr Harish Mithiran evaluates whether a tumour is suitable for minimally invasive surgery, such as Video-Assisted Thoracoscopic Surgery (VATS) or Robotic-Assisted Thoracic Surgery (RATS). These approaches can offer smaller incisions, less pain, shorter hospital stays, and faster recoveries in selected early-stage tumours. Open surgery remains important for larger or more complex masses involving nearby structures. The key principle is complete and safe removal, not simply choosing the smallest incision.

Recovery from a thymectomy depends on the extent of surgery and on whether chemotherapy or radiotherapy is also required. Hospital stay varies with the surgical approach and the extent of resection. After a thymectomy, patients usually need pain control, breathing exercises, early mobilisation, and follow-up to review the final pathology.
Recovery is often smoother after minimally invasive surgery, but all operations in this area require careful planning because the thymus lies close to the heart, major veins, lungs and nerves. If the pathology shows invasive disease or close margins, adjuvant treatment may be recommended.
Thymic carcinoma often recurs, while thymoma can recur even years after treatment, which is why long-term or lifelong follow-up may be needed. The best way to reduce the risk of recurrence is to aim for a complete initial treatment, follow through with recommended adjuvant therapy when indicated, and keep regular surveillance appointments afterwards.
Neumark helps by turning a rare and confusing diagnosis into a clear treatment plan.
We specialise in minimally invasive thoracic surgery with a multidisciplinary approach led by Dr Harish Mithiran, senior consultant thoracic surgeon at Gleneagles and Mount Alvernia hospitals. For patients with thymic cancer, we offer a careful review of imaging, an assessment of whether surgery is appropriate, coordination with oncology and radiology specialists as needed, and selection of the safest approach for tumour removal, or if a combined treatment plan is more appropriate.
If you have been told you may have thymic cancer or a mediastinal mass near the thymus, contact Neumark for a consultation today. Early specialist assessment can help clarify the diagnosis, explain your options, and guide you towards an optimal thymic cancer treatment plan without unnecessary delays.