

Thymoma and thymic carcinoma are both rare thymic cancers, but they differ significantly in their behaviour and appearance. Thymomas are generally slow-growing, resemble normal thymus cells, and rarely spread. Thymic carcinomas, unfortunately, are more aggressive, look different from normal cells, grow faster, and often metastasise, often leading to a poorer prognosis for the patient.
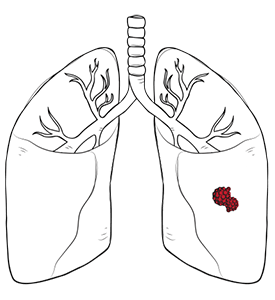
Thymic carcinoma cells are cancerous and tumour cells that appear more abnormal, usually grow faster with an aggressive growth pattern, and spread more readily to lymph nodes, the lining around the lungs or heart, or more distant parts of the body. When cancer spreads, tumour cells may reach distant sites via the lymphatic system and blood vessels. This is why it is more difficult to treat than thymoma.
The differences between thymoma and thymic carcinoma matter because the two diseases may arise from the same region but behave differently.
Another useful distinction is that thymoma is much more strongly associated with paraneoplastic syndromes and autoimmune diseases, such as myasthenia gravis. In practice, thymoma may be discovered because of muscle weakness, paraneoplastic syndromes, or another autoimmune problem, whereas thymic carcinoma is more often found because of a chest mass or imaging done for another reason.

Thymic carcinoma symptoms are often absent at first, but larger or more advanced tumours can cause pressure symptoms in the chest.
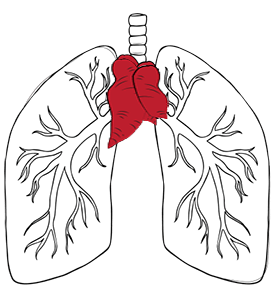
Many patients have no symptoms when the carcinoma is first found. In some cases, it is incidentally detected on a chest X-ray or CT scan. If symptoms do occur, they may include a cough that does not go away, shortness of breath, chest pain, hoarseness, or swelling of the face, neck, upper body, or arms. If these symptoms happen, it is because the tumour is pressing on nearby structures such as the airway, lung, major veins, or nerves in the chest.
As the symptoms can be vague, thymic carcinoma may be diagnosed later than thymoma.

You should see a thoracic specialist when imaging shows a thymic mass or when chest symptoms raise concern for a tumour in the anterior mediastinum.
A specialist review is important if the scan shows a thymic mass, an anterior mediastinal tumour, a thymoma, or a thymic carcinoma. It is also sensible to check with a doctor if you have persistent chest pain, breathlessness, a chronic cough, hoarseness, or swelling of the face and upper chest. Thymic carcinoma can resemble other conditions such as lymphoma, germ cell tumours, or metastatic cancer, and an expert review helps avoid both delay and the wrong treatment pathway.
A thoracic surgeon is often involved early, even before surgery is confirmed. This is because treatment planning depends on a range of factors that benefit from a surgeon’s expertise, such as whether the tumour appears to be removable, whether a biopsy is needed first, and whether nearby organs such as the pericardium, lung, or great vessels may be involved.
Thymic carcinoma is a heterogeneous group of rare thymic epithelial cancer malignancies.
Modern classifications recognise a broader range of thymic carcinoma subtypes and rare variants. Older literature used to categorise it more simply with a five-subtype model. In current practice, the most common subtype is squamous cell carcinoma. Other recognised thymic carcinoma subtypes include:
Each type of thymic cancer has its own specific features in the patient and under the microscope.
Some reported cancers are better understood as slight variations or patterns that overlap with existing types, rather than being completely new major ones. This distinction is important because not every descriptive phrase in a lab report means a completely new disease category.
Thymic carcinoma with neuroendocrine differentiation is a thymic cancer that shows features of hormone-producing cells and is grouped separately. Having these hormone-producing cell features in thymic carcinoma needs careful interpretation. Detailed genetic or molecular testing can sometimes help confirm the diagnosis or identify potential treatment targets. Examining tissue under a microscope to assess histology remains the primary method we use to classify these diseases.
The staging on how far the cancer has spread, treatment, and the expected outcome or prognosis are different for thymoma and thymic carcinoma. Thymic carcinoma is harder to treat than thymoma and typically has a less favourable prognosis. Both thymoma and thymic carcinoma can come back after treatment. Managing both thymoma and thymic carcinoma requires specialised doctors who are experts in chest tumours.

The management of thymic carcinoma often includes cancer treatments such as chemotherapy, radiation therapy, targeted therapies, or combinations of these therapies, especially when surgery is not possible or not enough on its own. Thymic carcinoma treatment options include standard treatment with chemotherapy and radiation therapy.
If the tumour is unresectable, locally advanced metastatic disease, or recurrent, non-surgical cancer treatments become central. Standard treatment with chemotherapy is commonly used to eradicate cancer cells while attempting to spare T cells and healthy tissue. Radiation therapy may be used after surgery when there is a concern for residual disease or as part of the definitive treatment. In the early stages of the disease, radiation therapy combined with surgery may remove the entire tumour.
New cancer treatments under study in thoracic oncology include immunotherapy and targeted agents. Treatment decisions depend on other factors, including the tumour biology and the patient’s fitness.

Thymic carcinoma surgery is considered when the tumour can be removed safely and completely, often as part of a broader treatment plan.
Surgery offers the best chance of durable disease control if complete removal is achievable. The operation usually involves removing the thymus and tumour together, often with surrounding fatty tissue and, if necessary, parts of any nearby involved structures. In some patients, this may mean removing a small portion of the lung, pericardium, or pleura, or an involved nerve or vein, to achieve complete removal of the carcinoma. The goal is not simply to remove a visible lump but to clear the disease as fully as possible.
Not every situation is ideal for minimally invasive surgery. Early and well-contained tumours may sometimes be approached with Video-Assisted Thoracoscopic Surgery (VATS) or Robotic-Assisted Thoracic Surgery (RATS) in experienced hands, but larger or invasive thymic carcinomas often require an open operation for safe exposure and complete removal.
At the Neumark Lung & Chest Surgery Centre, Dr Harish Mithiran uses minimally invasive thoracic techniques where appropriate, but the choice of approach is guided by the tumour stage, anatomy and oncologic safety rather than by the incision size alone.

Recovery after treatment for thymic carcinoma depends on the tumour stage, treatment type, and whether nearby structures are involved.
After surgery, patients usually need pain control, breathing exercises, early mobilisation, and follow-up to review the final pathology. The risks may include bleeding, infection, pain, air leaks, pneumonia, heart rhythm changes, or complications related to operating near the heart, great vessels, lungs, and phrenic nerves, all of which depend on the extent of the operation. Your surgeon will brief you on which symptoms are relevant to you and which warrant immediate treatment. If chemotherapy or radiotherapy is also needed, recovery can take longer and may involve a phased treatment plan rather than a single procedure.
Long-term follow-up is essential because thymic carcinoma has a higher risk of recurrence than thymoma. Follow-up usually includes repeat imaging and ongoing review by your treatment team. That matters not only for recurrence detection, but also for managing the longer-term effects of surgery, chemotherapy and/or radiotherapy.

Our experienced professionals at Neumark Lung & Chest Surgery Centre can turn a rare and complex diagnosis into a clear, personalised treatment plan. We specialise in minimally invasive thoracic surgeries with a multidisciplinary approach led by Dr Harish Mithiran, senior consultant thoracic surgeon at Gleneagles and Mount Alvernia hospitals.
For patients with thymic carcinoma, this means a careful review of imaging, thoughtful assessment of whether a biopsy or surgery should come first, and careful coordination of surgery with your oncologist and other specialists if a multimodal treatment plan is needed. Neumark’s published approach emphasises tailored care for mediastinal tumours, using VATS or robotic techniques where appropriate, while prioritising complete and safe tumour removal.
If you have been told you may have thymic carcinoma, or if a scan has shown a thymic mass and you are unsure what to do next, contact Neumark Lung & Chest Surgery Centre for a consultation. Early specialist input can clarify the diagnosis and help you move forward with the most appropriate treatment plan.