

A mediastinal mass is an abnormal growth in the mediastinum, the middle compartment of the thoracic cavity. The mass in front of the heart (the anterior mediastinum) includes the thymus gland and lymph nodes. Anterior mediastinal masses are the most common in adults and are often found incidentally while scanning for a different issue or during an investigation of chest symptoms.
Masses in the anterior mediastinum are more likely to be malignant, especially in older adults, so early detection and proper treatment are key.

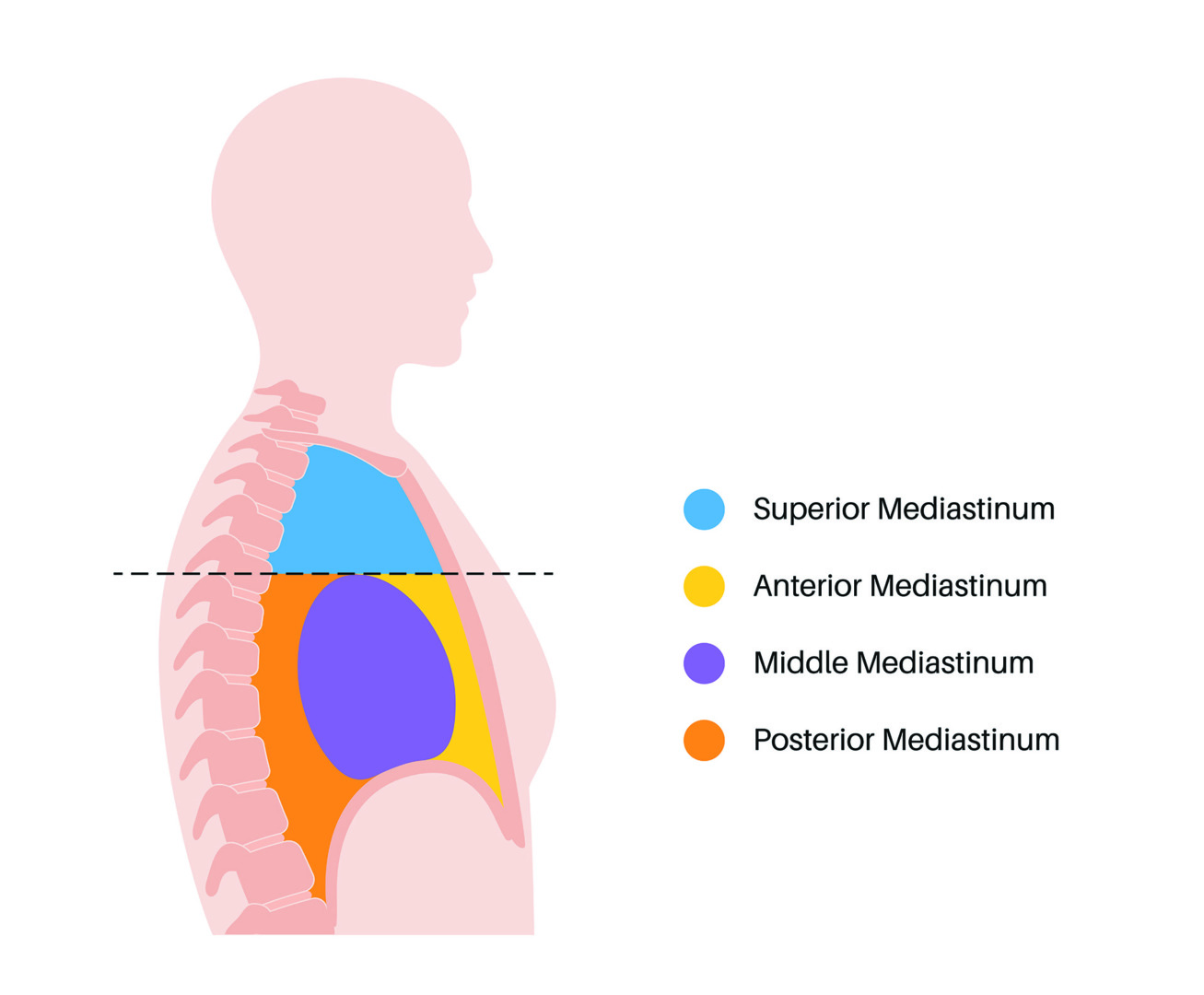
Anatomy of the Anterior Mediastinum
The anterior compartment is one of the three parts of the mediastinum, along with the middle and posterior. This region is the most forward part of the mediastinum and is bounded by the sternum anteriorly and the pericardium and great vessels posteriorly.
This compartment has several essential structures, such as the thymus gland, lymph nodes and thyroid tissue. The thymus gland is more prominent in younger individuals and plays a significant role in the immune system. Lymph nodes in this area are part of the body’s lymphatic system, which fights infections. The thyroid tissue can also extend into the anterior mediastinum, especially in substernal thyroid goitres. The nuances of this anatomy have a massive impact on diagnosing and managing anterior mediastinal masses.
Anterior Mediastinal Mass Causes
The most common causes of anterior mediastinal masses are thymomas, teratomas, lymphomas and substernal thyroid goitres. Thymomas – tumours of the thymus gland – are the most common. They are often associated with autoimmune disorders like myasthenia gravis, lupus or rheumatoid arthritis. Benign teratomas, another common cause, are diagnosed through imaging and often have intralesional fat, calcifications and varying tissue types.
Other causes include germ cell tumours like seminomas and non-seminomatous tumours, which may arise from embryonic tissue. Even though it is rare, fibrosing mediastinitis, a condition where fibrous tissue infiltrates the mediastinum, can also occur in the anterior area. Each condition has its clinical challenges. Many require imaging, biopsy and sometimes surgery to confirm the diagnosis and treatment plan.

Anterior vs Posterior Mediastinal Mass
Comparing anterior versus posterior mediastinal masses helps clinicians narrow down the diagnosis. While anterior masses have their own set of aforementioned causes, the posterior mediastinum is more common for neurogenic tumours, which arise from peripheral nerves and are more common in younger patients.
Anterior masses are more symptomatic because they are closer to vital organs like the heart and great vessels, and are more likely to be malignant. Posterior masses, although often benign, may still require surgical removal if there is spinal involvement or a risk of compression.
Symptoms and When to Investigate
Anterior mediastinal mass symptoms can range from mild to severe respiratory or cardiovascular symptoms. Common symptoms are chest pain, shortness of breath, persistent cough, and fullness in the chest. In some cases, the mass may compress the superior vena cava, leading to SVC Syndrome, a medical emergency which includes facial swelling, neck vein distension, and difficulty breathing.
Anterior mediastinal masses can also cause pleural effusion due to the compression or invasion of the pleural space. This may result in respiratory compromise that requires fluid drainage for symptomatic relief.
When systemic symptoms like unexplained weight loss, night sweats, or a fever accompany these local symptoms, a malignancy like lymphoma should be suspected. Some may have no symptoms, and the mass is discovered through imaging for unrelated reasons.

History and Physical Examination
A thorough history and physical examination is essential for evaluating patients with anterior mediastinal masses, as these can provide critical clues to the underlying diagnosis. Your medical specialist will look into your medical history and ask detailed questions about symptoms like chest pain, cough and shortness of breath, as well as any history of autoimmune diseases or cancer. They will then do a thorough physical examination of the chest and abdomen, and a neurological exam to check for any signs of spinal cord compression.
Imaging and Diagnosis
Initial evaluation often starts with a chest X-ray, which is usually followed by a CT scan, which provides a detailed view of the mass’s size, shape and relationship to surrounding structures. An anterior mediastinal mass CT scan is one of the most important tools for assessing the extent of the tumour and planning the next steps. An MRI is used when better soft tissue contrast is needed, and PET-CT helps assess metabolic activity and guide biopsy. Tissue sampling is usually required for a definitive diagnosis.
Depending on the tumour’s accessibility, an anterior mediastinal mass biopsy can be performed using CT-guided techniques, EBUS (endobronchial ultrasound), or mediastinoscopy.
Proper biopsy technique is crucial as small or necrotic samples may not provide enough information to differentiate between tumour types. A multidisciplinary review is often recommended to interpret the findings in a clinical context.

Surgical Treatment with RATS and VATS
Robotic-Assisted Thoracoscopic Surgery (RATS) and Video-Assisted Thoracoscopic Surgery (VATS) have revolutionised the treatment of anterior mediastinal tumours, such as thymomas, benign teratomas and germ cell tumours, by offering minimally invasive options with fewer complications and faster recovery.
RATS offers 3D visualisation and precise instrument control, making it ideal for complex resections in confined spaces like the anterior mediastinum. It allows for smaller incisions, less post-operative pain and quicker discharge while maintaining excellent oncological control.
VATS is another option, especially for smaller, well-demarcated tumours. It involves inserting a camera and specialised instruments through small incisions to remove the mass. VATS is suitable for patients who are not candidates for more invasive procedures due to age or comorbid conditions.
In both cases, surgical planning is highly individualised and based on tumour type, location and patient health. The goal is complete resection while preserving surrounding structures.

Prognosis and Survival Rate
The anterior mediastinal mass survival rate depends on several factors, including the type of tumour, stage at diagnosis and treatment approach. For example, encapsulated thymomas have a 5-year survival rate of 96–100% while invasive or metastatic thymomas have a variable outcome of 11% to 50%.
Germ cell tumours also have different prognoses. Teratomas generally have a good prognosis, while non-seminomatous tumours may require surgery and chemotherapy. Lymphomas, depending on their subtype, respond well to chemotherapy and radiation but need long-term follow-up.
Regardless of the type of mass, early detection, complete surgical resection, and appropriate adjunctive therapies all improve survival.

Anterior Mediastinal Mass Complications
Due to their location, anterior mediastinal masses can cause significant complications. One primary concern is compression of adjacent structures, including the trachea, bronchi, oesophagus and major blood vessels like the superior vena cava. SVC syndrome can develop rapidly and requires urgent medical attention.
In addition to cardiac compression, airway obstruction and even spinal cord involvement may occur, especially if the tumour is large or invasive. In malignant cases, there is also the risk of local invasion and distant metastasis, which complicates treatment and worsens prognosis.
Minimally invasive surgical approaches reduce the risk of operative complications, but proper pre-operative imaging and planning are important to avoid intraoperative surprises when treating anterior mediastinal masses.

Preventing Recurrence
Even after treatment, anterior mediastinal mass recurrence is possible, especially in malignant or incompletely resected tumours. For this reason, ongoing surveillance with imaging is important. Depending on the tumour type and recurrence risk, follow-up may involve periodic CT or PET-CT scans.
In cases with high recurrence risk, adjuvant therapy – such as chemotherapy or radiotherapy – may be added to the surgical approach to improve long-term control. A well-structured follow-up plan overseen by a thoracic specialist ensures early detection of any recurrence and timely intervention.

Expert Thoracic Care at Neumark
Managing an anterior mediastinal mass requires a multidisciplinary approach and high surgical expertise. At Neumark Lung & Chest Surgery Centre, patients receive state-of-the-art care from a team specialising in minimally invasive thoracic procedures, comprehensive imaging and personalised treatment planning.
Whether you are newly diagnosed or seeking a second opinion, Neumark offers compassionate, patient-centred care to achieve the best possible outcomes. Our thoracic surgeon and lung specialist in Singapore are committed to providing precise diagnosis, advanced surgical options, and long-term support.
If you have been diagnosed with an anterior mediastinal mass or are experiencing unexplained chest symptoms, contact us today for expert evaluation and tailored treatment options.