

Understanding Mediastinal Masses
Mediastinal masses are abnormal growths in the mediastinum, the central compartment of the chest. They can be benign or malignant and arise from any of the tissues or organs in the mediastinum. A middle mediastinal mass often presents with distinct symptoms and treatment implications, necessitating an accurate diagnosis. Importantly, early detection and management are crucial for achieving better outcomes with middle mediastinal masses.
What Is The Mediastinum?
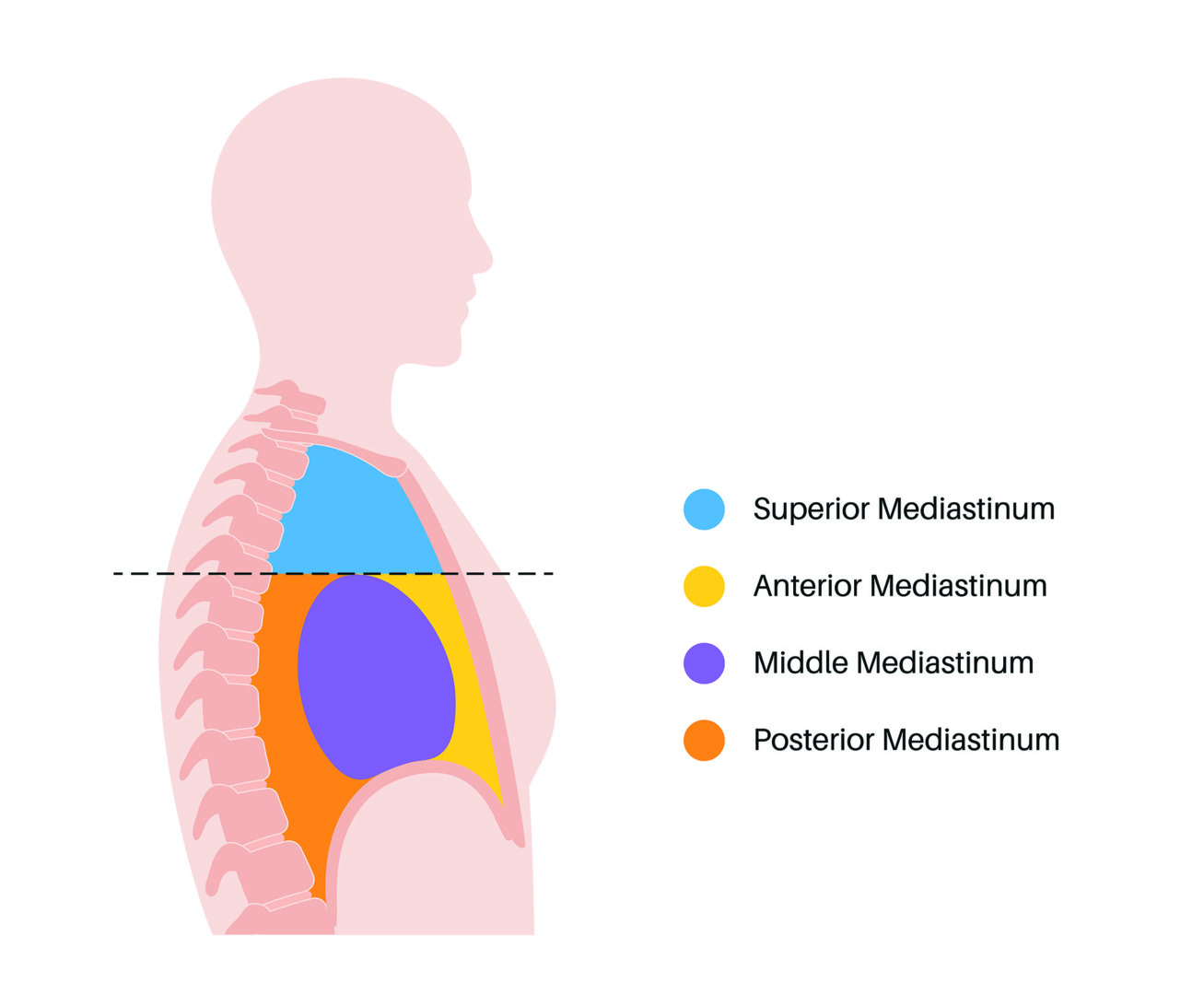
The mediastinum is divided into three parts, each containing different anatomical structures and associated with specific types of masses. For clinical purposes, it is divided into three parts: anterior, middle and posterior. The middle compartment of the chest is between the lungs and is bordered by the sternum in front and the spine at the back.
Understanding the mediastinum’s anatomy helps clinicians localise the mass and guide treatment. While masses can occur in any compartment, those in the middle mediastinum require particularly careful evaluation as this space is complex and densely packed. Specifically, the middle mediastinum contains the heart, major vessels like the superior vena cava, and tracheobronchial lymph nodes.
What Is A Middle Mediastinal Mass?
A middle mediastinal mass is any abnormal growth or enlargement in the central compartment of the mediastinum. This area includes the trachea, main bronchi, heart, great vessels (aorta and pulmonary arteries), oesophagus, and various lymph nodes. The mass can be congenital, inflammatory, infectious or neoplastic.
Common middle mediastinal masses include:
- Bronchogenic cysts: benign congenital lesions that can compress adjacent structures
- Lymphadenopathy: often related to infection, inflammation or malignancy, including tuberculosis
- Vascular lesions: aneurysms or vascular malformations
- Metastatic cancers or lymphomas
- Fibrosing mediastinitis: dense fibrosis that encases and obliterates the lumen of mediastinal vessels and airways
Carcinomas such as squamous cell carcinoma of the oesophagus and thymic carcinoma can also present as malignant middle mediastinal masses. Middle mediastinal masses are more likely to be benign than anterior masses; however, this doesn’t diminish their clinical significance, especially if they cause symptoms or obscure diagnosis.
Middle Mediastinal Mass Symptoms
The symptoms of a middle mediastinal mass depend on its size, location and effect on adjacent structures. Since the middle mediastinum is home to critical components of the cardiovascular and respiratory systems, even a benign lesion can produce significant symptoms.
Patients may experience:
- Persistent coughing
- Shortness of breath or wheezing
- Chest discomfort or pain
- Difficulty swallowing (dysphagia)
- Hoarseness due to recurrent laryngeal nerve involvement
- Superior vena cava (SVC) syndrome occurs if vascular compression occurs
These symptoms often prompt imaging studies that reveal the presence of a mass, leading to further diagnostic evaluation. A diagnosis starts with a detailed medical history and physical examination, followed by advanced imaging. A chest X-ray may provide initial evidence, but CT scans offer more detailed cross-sectional views to assess the size, shape, and impact on surrounding tissues.
In some cases, an MRI is preferred, especially when vascular involvement is suspected or when radiation exposure is a concern. PET scans may also evaluate metabolic activity to distinguish between benign and malignant lesions.
Once imaging is complete, a multidisciplinary team of radiologists, thoracic surgeons and oncologists reviews the findings to formulate a diagnostic and treatment plan. In many cases, a biopsy may be necessary to better prepare for middle mediastinal mass treatment.

Biopsy of Middle Mediastinal Mass
The method of biopsy chosen depends on the mass’s location, size and suspected nature. Options include:
- Endobronchial ultrasound-guided biopsy (EBUS): helpful in sampling lymph nodes
- CT-guided needle biopsy: for accessible lesions
- Mediastinoscopy: a surgical procedure to obtain tissue when other approaches are inconclusive
Each biopsy method has benefits and risks, and the choice is tailored to each patient. A definitive tissue diagnosis enables clinicians to determine whether surgery, medical therapy, or observation is the most suitable course of action.

Surgical Management of Middle Mediastinal Tumours
Robotic-Assisted Thoracoscopic Surgery (RATS) and Video-Assisted Thoracoscopic Surgery (VATS) have revolutionised the management of middle mediastinal masses, including bronchogenic cysts, enlarged lymph nodes, and other benign or malignant lesions. These minimally invasive techniques provide a safer and more refined approach to operating in this complex and crowded region of the chest.
RATS provides surgeons with 3D visualisation and highly responsive instrument control, particularly beneficial when working around critical structures, such as the heart, trachea, oesophagus, and great vessels in the middle mediastinum. This precision allows for smaller incisions, reduced trauma to surrounding tissue, and shorter hospital stays, all without compromising oncological effectiveness.
VATS is very valuable, particularly for well-defined and smaller middle mediastinal masses. Using a thoracoscopic camera and long instruments inserted through small keyhole incisions, VATS enables surgeons to remove the mass while avoiding a full thoracotomy, making it ideal for older patients or those with significant comorbidities.
In both approaches, surgical planning is tailored to individual factors such as tumour type, location and overall patient health, which guide decision-making. The ultimate aim is complete and safe resection while preserving vital anatomical structures and ensuring the best possible outcome.

Prognosis and Follow-Up
Prognosis and the follow-up of mediastinal masses depend on the underlying cause and treatment. Benign masses, such as thymic cysts or duplication cysts, have a better prognosis than malignant masses, like non-Hodgkin lymphoma or germ cell tumours.
Regular follow-up imaging studies, such as CT scans or MRIs, are crucial for monitoring the size and composition of the mass and detecting any changes or complications. These studies will ensure that any recurrence or progression of the mass is detected early and can be treated promptly.
In some cases, additional testing, such as a biopsy or blood work, may be required to confirm the diagnosis or to monitor the response to treatment. Management of mediastinal masses often involves a multidisciplinary approach including surgery, chemotherapy and radiation therapy. Prognosis and the follow-ups should be individualised based on the characteristics of the mass and the patient’s overall health.
By combining regular monitoring with a tailored treatment plan, healthcare providers can optimise outcomes for patients with mediastinal masses. At Neumark Lung & Chest Surgery Centre, we provide comprehensive care and support throughout the diagnostic and treatment process.

When to See a Thoracic Surgeon
Anyone diagnosed with a middle mediastinal mass or experiencing symptoms such as unexplained chest pain, a persistent cough or difficulty breathing should see a thoracic surgeon promptly. Early evaluation is essential to determine the nature of the mass and whether surgery is required.
Even benign lesions can grow or cause complications if left untreated. A thoracic surgeon can assess your condition, recommend imaging tests or a biopsy, and explain your options, including whether a minimally invasive approach is suitable.
Neumark Lung & Chest Surgery Centre combines surgical expertise with patient-centred care to manage middle mediastinal masses. Whether you need further workup or a comprehensive surgical plan, we’re here to help.
Don’t wait for your symptoms to get worse. Contact us today to book a consultation and begin your journey to clarity, confidence, and improved breathing.