

The immune system produces abnormal antibodies that target the acetylcholine receptor. The most common are antibodies to the acetylcholine receptor. Other abnormal antibodies include muscle-specific kinase (MuSK) and LRP4. Myasthenia gravis is an autoimmune disease, meaning the immune system mistakenly targets the neuromuscular junction.
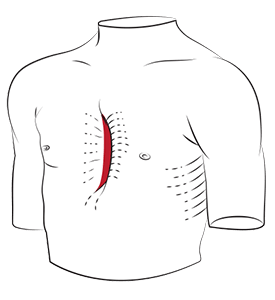
The thymus gland plays an important role for many people with myasthenia gravis. The thymus gland sits in the front of the chest behind the breastbone. In some cases of myasthenia gravis, the thymus gland shows thymic hyperplasia (enlargement) or thymic abnormalities. Thymus gland tumours can also be associated with MG. Risk factors include thymic hyperplasia, autoimmune conditions and family history.
MG is not the same as congenital myasthenia or congenital myasthenic syndromes, which are rare diseases caused by genetic defects at the neuromuscular junction rather than an immune system attack. Neonatal myasthenia gravis is a transient condition that occurs in newborns of mothers with MG when maternal antibodies cross the placenta. Unlike congenital myasthenia, neonatal myasthenia is temporary. Transient neonatal MG usually resolves as neonatal myasthenia improves over the course of weeks.
Many wonder whether myasthenia gravis is genetic. MG is not usually inherited in a simple way. Some families may have a higher risk of autoimmune disease and of immune cells mistakenly attacking healthy cells, but most cases occur without a clear hereditary pattern.

Myasthenia gravis symptoms often involve fatigable muscle weakness that worsens with activity. Signs and symptoms vary depending on which muscle groups myasthenia gravis affects.
The earliest signs and symptoms of myasthenia gravis commonly involve the muscles of the eye. Ocular myasthenia gravis includes droopy eyelids (on one eye or both), double vision or blurred vision, especially later in the day. MG affects facial expression, chewing, swallowing, and speech. Some people with myasthenia gravis experience a nasal voice or slurred speech after prolonged talking. Difficulty swallowing is another symptom.
Other myasthenia gravis symptoms include head drop, difficulty holding arms up, trouble climbing stairs, and muscle fibres ‘giving out’ with repeated use. Heat, infection, stress, and certain medications are risk factors that worsen MG symptoms. One common symptom of MG is fatigue that builds throughout the day.
A key risk to understand is myasthenic crisis. This is severe muscle weakness affecting the breathing muscles, potentially leading to respiratory failure. Seek urgent care if you develop shortness of breath at rest, difficulty swallowing, choking, or a rapid worsening of muscle weakness.
You should see a lung specialist or thoracic surgeon when myasthenia gravis is associated with thymus gland disease, or when a thymectomy is being considered.
Thoracic input becomes important when imaging suggests thymus gland abnormalities, when a thymoma is suspected, or when thymectomy for MG is part of the plan for selected patients with generalised myasthenia gravis.
You may also be referred to a thoracic team if you have recurrent chest infections related to swallowing problems, or if there is concern about respiratory muscle weakness and the need for coordinated perioperative planning for the medical procedures.
In Singapore, patients often present to thoracic review after a chest CT identifies thymic enlargement or a thymic mass. Some are referred by a neurologist or from a hospital emergency visit after a significant flare-up.

The non-surgical management of myasthenia gravis focuses on improving muscle strength and reducing an immune-mediated attack. The goal is to improve muscle weakness and manage symptoms.
Many patients start with cholinesterase inhibitors, such as pyridostigmine, which improve the neuromuscular transmission. Cholinesterase inhibitors can improve muscle weakness but do not change the underlying immune system process. If symptoms persist, treatment may include corticosteroids and immunosuppressive therapies targeting the immune system and its cells. Certain medications, such as beta blockers, can worsen MG and should be discussed with your doctor.
Some people with myasthenia gravis need faster-acting therapies during a severe flare-up or crisis. Intravenous immunoglobulin and plasma exchange can provide rapid improvement by removing abnormal circulating antibodies. MG treated with these therapies may see rapid improvement in muscle weakness.
Practical self-management matters too. Many with myasthenia gravis experience improved muscle strength when they learn to pace activity, plan more demanding tasks earlier in the day, and take rest breaks before muscle fatigue becomes severe. Treat any infections early, maintain a regular sleep schedule, and discuss vaccination timing with your doctor. Tell any doctor or dentist that you have MG, because some medicines can worsen myasthenia gravis symptoms.
Newer immune therapies are available to treat myasthenia gravis in people who do not respond to conventional treatments. Speak with a specialist about these therapies and whether they are viable for you.

Surgery for myasthenia gravis usually involves a thymectomy, which is the removal of the thymus gland. A thymectomy may be recommended for two main reasons:
Thymectomy is not an emergency procedure. It is planned when MG symptoms are reasonably stable and when perioperative risks can be managed. Our team at Neumark will coordinate the timing with your neurologist, especially if you are on steroids or other immunosuppressants. They may use preoperative therapies such as intravenous immunoglobulin or plasma exchange in selected higher-risk cases.
Myasthenia gravis thymectomy can be performed using open or minimally invasive approaches, depending on the thymus gland anatomy and the surgeon’s judgment.
Minimally invasive techniques may include VATS, RATS, or U-VATS, which use small incisions and a camera. These approaches can support recovery by reducing chest wall trauma.
At Neumark, Dr Harish Mithiran discusses the options and what recovery looks like. Procedures are performed at Gleneagles Hospital or Mount Alvernia Hospital.

Most people with myasthenia gravis recover well, but MG requires careful perioperative planning to reduce any respiratory failure and swallowing risks. Any thymectomy carries risks such as bleeding, infection, pneumonia, pain, and, rarely, injury to nearby structures. Specific concerns include the phrenic nerve, which innervates the diaphragm, and postoperative respiratory muscle weakness in patients with uncontrolled MG.
Recovery depends on your baseline muscle strength. With minimally invasive surgery, hospital stays are often shorter. You may still experience muscle fatigue for several weeks.
Your team will also monitor for worsening postoperative myasthenia. Some patients with myasthenia gravis experience temporary fluctuations in symptoms in the weeks after surgery, and medication adjustments may be needed. The benefits of thymectomy, when it is appropriate, often develop gradually over months rather than immediately.
Most patients with myasthenia gravis can live well by combining medical treatment with pacing and trigger awareness. People achieve better outcomes when they proactively manage their MG symptoms.
Plan demanding activities for times when you are strongest, and build rest into the day. Heat can worsen muscle weakness, so stay cool during Singapore’s hotter months and consider indoor exercise options when MG symptoms flare up. If swallowing is affected, modify food texture and eat slowly. Seek early review for chest infections and discuss any new medicines with your care team.
It is also normal to feel anxious when MG symptoms fluctuate. Know which symptoms warrant urgent care, keep your medication list up to date, and bring a family member to appointments if possible.
Myasthenia gravis life expectancy is usually near normal with modern treatment, but severe respiratory involvement and respiratory failure can be life-threatening without urgent care. The most serious complication is myasthenic crisis, where muscle weakness affects breathing muscles to the point that ventilatory support may be needed. With early recognition, hospital monitoring, and modern therapies, outcomes have improved markedly. Your specialist can explain your personal risk based on severity, antibody type, and past crises.
Neumark supports patients with myasthenia gravis who need thoracic assessment and surgery, especially for thymectomy and thymus gland tumours. Dr Harish Mithiran works closely with the neurology, anaesthesia and respiratory teams to ensure safe surgery and a structured recovery. If you have a thymic mass on imaging, have been advised to consider thymectomy, or want a clear explanation of surgical options, a consultation can help you understand the benefits, limitations, and next steps.
If you have been diagnosed with MG and have questions about thymus gland evaluation or myasthenia gravis thymectomy, contact Neumark Lung & Chest Surgery Centre to book a consultation at Gleneagles or Mount Alvernia hospitals in Singapore.