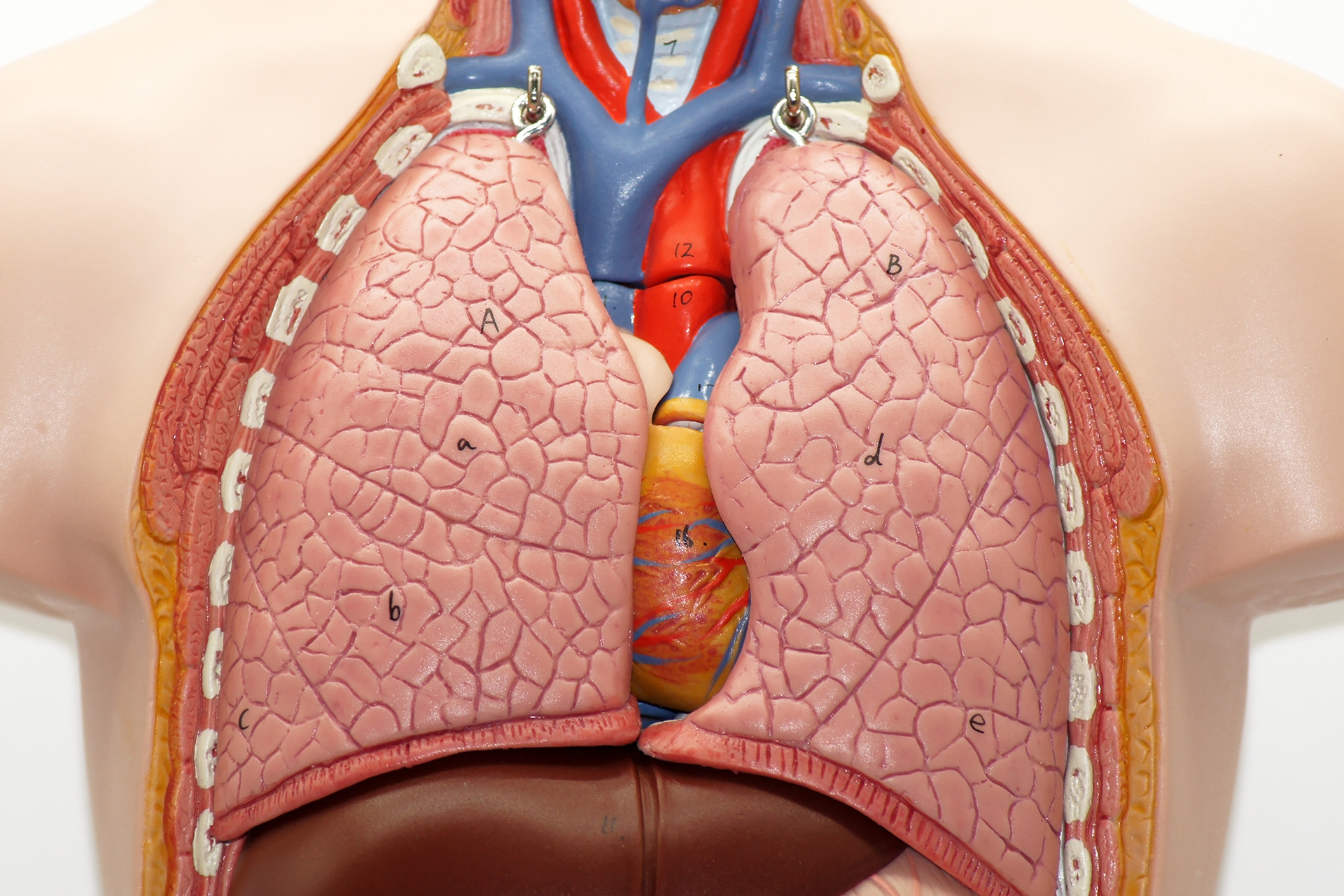



During lung decortication, the surgeon removes the thick pleural peel from the lung and clears infected or organised material from the pleural space.

After decortications, patients are closely monitored as the lung re-expands and fluid or air drains from the chest.
You may wake up with a chest drain, oxygen, a drip, and pain relief. Some patients need closer monitoring in a high-dependency or intensive care unit, especially after major infection, open surgery, or complex lung decortication.
Most patients stay in the hospital until the chest tubes are removed. Chest drains usually stay in place until air leakage settles and drainage reduces. Chest X-rays help check lung expansion. Nurses and physiotherapists will encourage deep breathing, coughing and early walking. These steps reduce the risk of pneumonia, blood clots and lung collapse.
Postoperative pain is expected, especially after a thoracotomy. Pain relief may include tablets, injections, nerve blocks, or an epidural, depending on the operation and your condition.
The main benefit of decortications is that a trapped lung can be re-expanded, thereby improving breathing.
Most patients feel less breathless once the lung opens more fully. Patients with thick scarring may see clear improvement. Decortications along the visceral pleura can also remove infected material, reduce the risk of ongoing sepsis, improve oxygen levels, and reduce the risk of a persistently infected pleural space.
Outcomes depend on the cause, the surgical technique chosen, and the health of the underlying lung. Patients with thick pleural scarring but relatively preserved lung tissue tend to benefit most. If the lung has a severe underlying disease, improvement may be more limited.
Pleural decortications do not always treat the underlying disease. For example, if a cancer caused the pleural problem, decortication may help with the symptoms, diagnosis, or lung expansion, but cancer treatment may still be needed. This may include chemotherapy, immunotherapy, targeted therapy, or radiation therapy, depending on the cancer type.
Decortication, as a surgical intervention, is a major thoracic surgery and carries risks such as bleeding, infection, air leak, pain, and incomplete lung expansion.
Possible postoperative complications include:
Haemorrhages can occur from raw lung surfaces after the thick peel is removed. Some patients may need a blood transfusion.
If any infected materials remain in the chest, a retained infective focus can lead to postoperative sepsis. Rarely, the lung may not expand well after surgery because the lung tissue itself is too damaged.

Recovery after decortication depends on the surgical approach, severity of disease, and how well the lung re-expands. Some patients stay several days, while more complex infections or open thoracic surgery may need longer monitoring. Recovery at home can take several weeks. Full recovery may take longer after a thoracotomy.
During recovery, patients are usually advised to walk regularly, continue breathing exercises, keep wounds clean and dry, avoid heavy lifting until cleared, and attend follow-up appointments. Follow-up imaging may be arranged to assess lung expansion and confirm that the pleural space is healing.
Call your doctor urgently if you develop a fever, worsening breathlessness, increasing chest pains, dizziness, wound redness, swellings, discharges, coughing up blood, or any sudden deterioration. These symptoms may suggest an infection, bleeding, air leaks, or another complication.
Alternatives to decortication may include antibiotics, thoracentesis, chest tube drainage, intrapleural medicines, an indwelling pleural catheter, pleurodesis, or ongoing monitoring.
The right alternative depends on the cause:
Neumark Lung & Chest Surgery Centre helps patients understand whether decortication is needed and which surgical approach is safest for their condition.
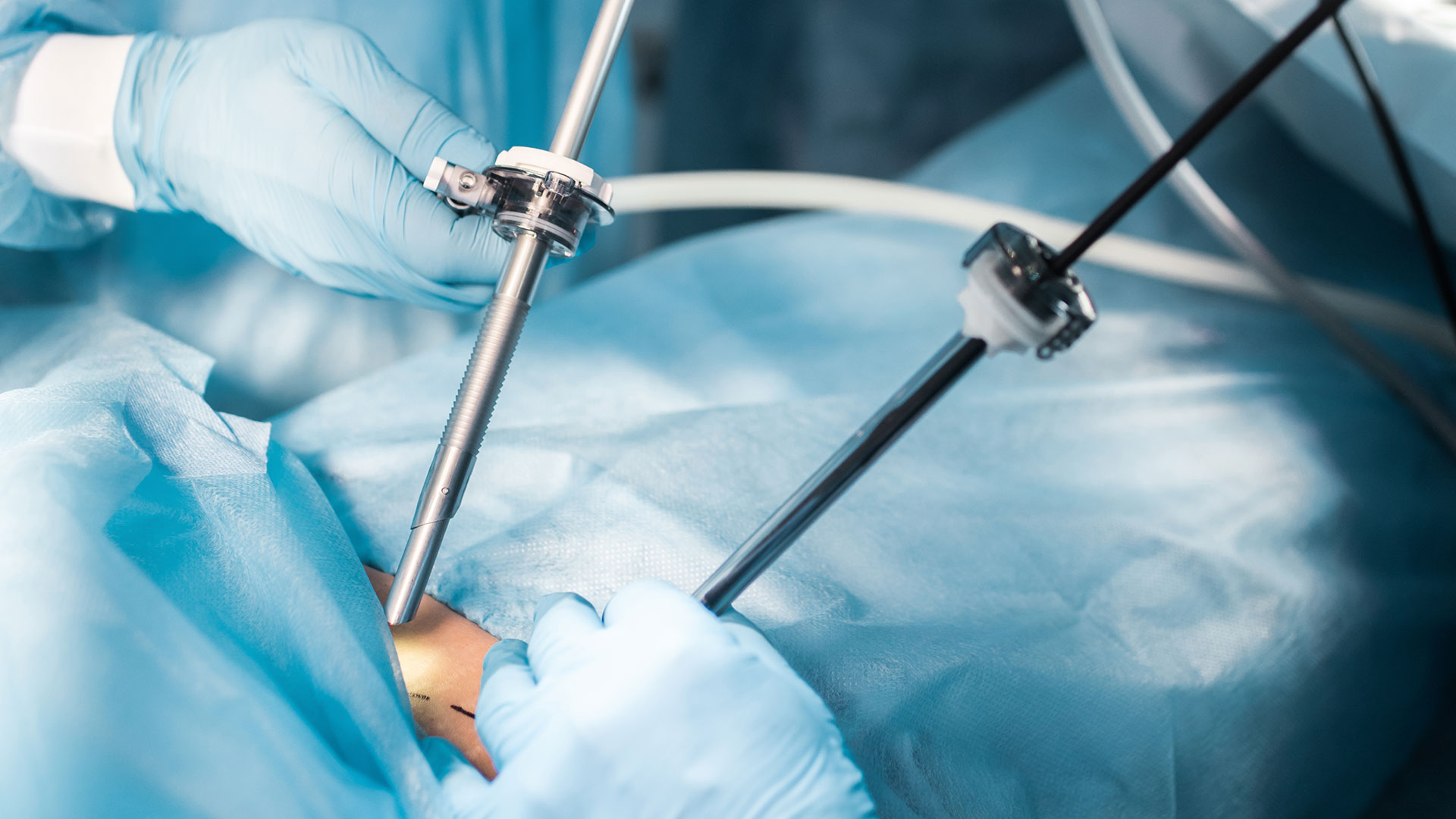
Neumark specialises in minimally invasive surgery, with a multidisciplinary approach led by Dr Harish Mithiran, senior consultant thoracic surgeon at Gleneagles and Mount Alvernia hospitals. For patients with restricted lung, empyema, pleural thickening, or complex pleural disease, this means careful review of symptoms, scans, fluid results, infection status, lung functions, and overall fitness.
If you have been told you have a trapped lung, chronic empyema, pleural thickening, or need decortication, contact Neumark today for a consultation.